What Are the New Findings?
The number of medical evacuations for battle injuries has decreased considerably since 2014. Most medical evacuations in 2018 were attributed to mental health disorders, followed by non-battle injury/poisoning; signs, symptoms, and ill-defined conditions; musculoskeletal disorders; and digestive system disorders.
What Is the Impact on Readiness and Force Health Protection?
Medical evacuations have a significant impact on military readiness because of loss of personnel and the resultant effects on unit cohesion and mission effectiveness. In addition, the costs of medical evacuations related to non-battle injuries are considerable. Military medical providers should continue to apply pre-deployment screening processes to optimize service members' medical and psychological fitness to deploy.
Background
Although there have been substantial reductions in combat operations taking place in the U.S. Central Command (CENTCOM) area of responsibility (AOR) in Southwest Asia,1–5 the number of service members deployed to the CENTCOM AOR is still significant. Reports indicate that there are currently about 14,000 to 15,000 service members in Afghanistan for Operation Resolute Support and another 2,000 reinforcing the Syrian Democratic Forces.6–8 In theaters of operations such as Afghanistan, most medical care is provided by deployed military medical personnel; however, some injuries and illnesses require medical management outside the operational theater. In these cases, the affected individuals are usually transported by air to a fixed military medical facility in Europe or the U.S. where the service members receive the specialized, technically advanced, and/or prolonged diagnostic, therapeutic, and rehabilitative care required.
Medical air transports, or medical evacuations, are costly and generally indicative of serious medical conditions. Some serious conditions are directly related to participation in or support of combat operations (e.g., battle wounds); however, many others are unrelated to combat and may be preventable. This report summarizes the natures, numbers, and trends of conditions for which male and female military members were medically evacuated from CENTCOM AOR operations during 2018 and compares them to the previous 4 years.
Methods
The surveillance period was 1 Jan. 2014 through 31 Dec. 2018. The surveillance population included all members of the active and reserve components of the U.S. Army, Navy, Air Force, and Marine Corps who were deployed to the CENTCOM AOR during the period. The outcome of interest in this analysis was medical evacuations during the surveillance period from the CENTCOM AOR (e.g., Afghanistan or Iraq) to a medical treatment facility outside the CENTCOM AOR. Records of all medical evacuations conducted by the U.S. Transportation Command (TRANSCOM) maintained in the TRANSCOM Regulating and Command & Control Evacuation System (TRAC2ES) were utilized. Evacuations were included in the analyses if the affected service member had at least 1 inpatient or outpatient medical encounter in a permanent military medical facility in the U.S. or Europe during a time interval extending from 5 days before to 10 days after the reported evacuation date.
Medical evacuations included in the analyses were classified by the causes and natures of the precipitating medical conditions (based on information reported in relevant evacuation and medical encounter records). First, all medical conditions that resulted in evacuations were classified as "battle injuries" or "non-battle injuries and illnesses" (based on entries in an indicator field of the TRAC2ES evacuation record). Evacuations due to non-battle injuries and illnesses were subclassified into 17 illness/injury categories based on International Classification of Diseases, 9th/10th Revision, Clinical Modification (ICD-9-CM/ICD-10-CM) diagnostic codes reported on records of medical encounters after evacuation. For the purposes of this report, all records of hospitalizations and ambulatory visits from 5 days before to 10 days after the reported date of each medical evacuation were identified. In most cases, the primary (first-listed) diagnosis for either a hospitalization (if any occurred) or the earliest ambulatory visit after evacuation was considered indicative of the condition responsible for the evacuation. However, if the first-listed diagnostic code specified the external cause (rather than the nature) of an injury (ICD-9 E-code/ICD-10 V-, W-, X-, or Y-code) or an encounter for something other than a current illness or injury (e.g., observation, medical examination, or vaccination [ICD-9 V-codes/ICD-10 Z-codes other than those related to pregnancy]), then secondary diagnoses that specified illnesses and injuries (ICD-9 codes 001–999; ICD-10 codes A00–T88) were considered the likely reasons for the subject evacuations. If there was no secondary diagnosis or if the secondary diagnosis also was an external cause code, the first-listed diagnostic code of a subsequent encounter was used.
Deployment data were no longer available in the Defense Medical Surveillance System (DMSS) beginning in 2018; therefore, rates of medical evacuations per deployed person-time were not calculated. The disposition after each medical evacuation was determined by using the disposition code associated with the medical encounter that was used for documenting the category of the medical evacuation. Inpatient disposition categories were returned to duty (code 01), transferred/discharged to other facility (codes 02–04, 09, 21–28, 43, or 61–66), died (codes 20, 30, 40–42, 50, or 51), separated from service (codes 10–15), and other/unknown. Outpatient disposition categories were released without limitation (code 1), released with work/duty limitation (code 2), immediate referral (code 4), sick at home/quarters (codes 3 or S), admitted/transferred to civilian hospital (codes 7, 9, A–D, or U), died (codes 8 or G), discharged home (code F), and other/unknown.
Results
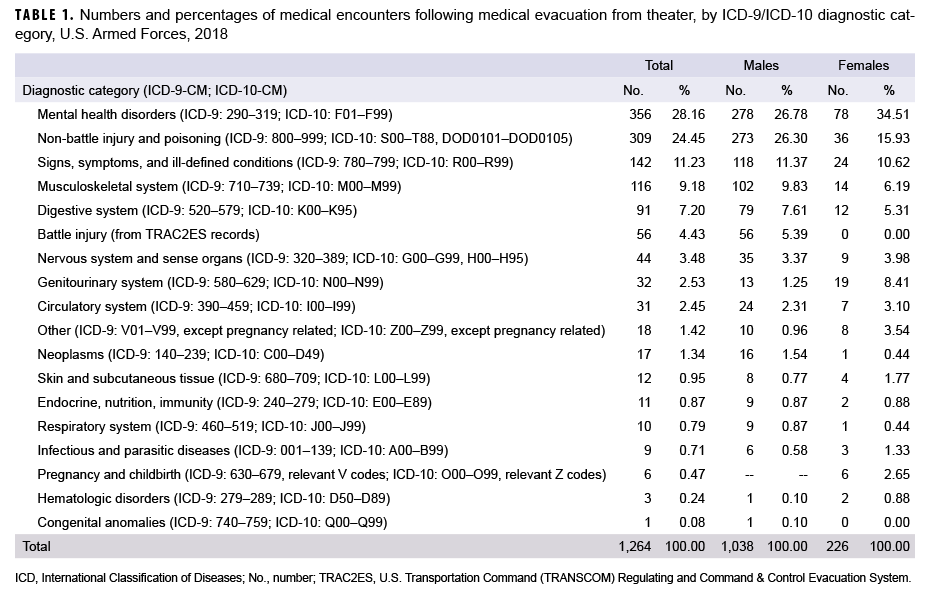
In 2018, a total of 1,264 medical evacuations of service members from the CENTCOM AOR were followed by at least 1 medical encounter in a fixed medical facility outside the operational theater (Table 1). Overall, there were more medical evacuations for mental health disorders (n=356; 28.2%) than for any other single category of illnesses or injuries (Table 1). In addition, the numbers of evacuations for non-battle injuries and poisonings (n=309; 24.5%); signs, symptoms, and ill-defined conditions (n=142; 11.2%); musculoskeletal system disorders (n=116; 9.2%); and disorders of the digestive system (n=91; 7.2%) were all higher than the number of evacuations for battle injuries (n=56; 4.4%). The top 3 categories—mental health disorders (most frequently adjustment and depressive disorders); non-battle injuries (primarily fractures of extremities, strains, and sprains); and signs, symptoms, and ill-defined conditions (primarily pain and swelling)—accounted for more than half (63.8%) of all evacuations (Table 1).
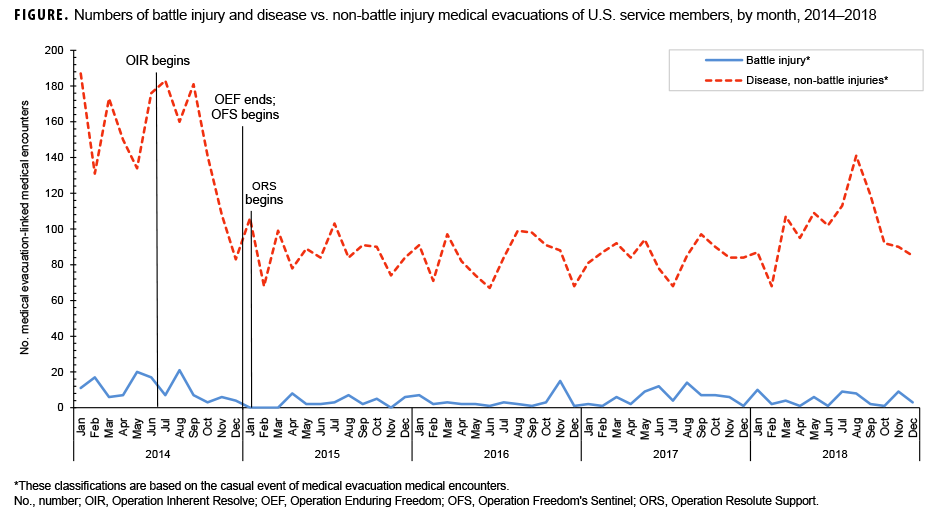
During 2014–2018, the annual number of medical evacuations attributable to battle injuries peaked in 2014 (n=126) then decreased in 2015 (n=35) and remained relatively low in 2016 (n=42) before increasing in 2017 (n=71) and decreasing again in 2018 (n=56) (data not shown). Over the 5-year period, the annual number of battle injury-related evacuations declined 55.6% from the peak year of 2014 through the most recent year, 2018. The annual number of medical evacuations attributable to non-battle injuries and diseases peaked in 2014 (n=1,807) and then decreased to relatively low levels in 2015 (n=1,050), 2016 (n=1,010), and 2017 (n=1,024) before increasing again in 2018 (n=1,208). In general, the annual numbers of medical evacuations over the course of the 5-year period varied in relation to the numbers of deployed service members, with the highest yearly count of medical evacuations occurring during the final year (2014) of Operation Enduring Freedom (OEF). The monthly numbers of medical evacuations decreased considerably in the later months of 2014 leading up to 1 Jan. 2015, when U.S. Forces-Afghanistan formally ended OEF and began Operation Freedom's Sentinel (OFS) (Figure).
Demographic and Military Characteristics
The number of medical evacuations in 2018 was higher among males (n=1,038) than females (n=226) (Table 1, 2). The most frequent causes of medical evacuations among male service members were mental health disorders (n=278; 26.8%); non-battle injury and poisoning (n=273; 26.3%); signs, symptoms, and ill-defined conditions (n=118; 11.4%); and musculoskeletal disorders (n=102; 9.8%) (Table 1). Among female service members, the most frequent causes of medical evacuations were mental health disorders (n=78; 34.5%); non-battle injury and poisoning (n=36; 15.9%); signs, symptoms, and ill-defined conditions (n=24; 10.6%); and genitourinary system disorders (n=19; 8.4%).
Compared to males, females had higher percentages of evacuations for about half of all illness and injury categories. Female service members had notably higher percentages of medical evacuations for mental health disorders and genitourinary system disorders compared to males (Table 1). In contrast, male service members had higher percentages of evacuation for injuries (both battle and non-battle related) and for musculoskeletal disorders. There were no medical evacuations of a female service member during 2018 for a battle injury.
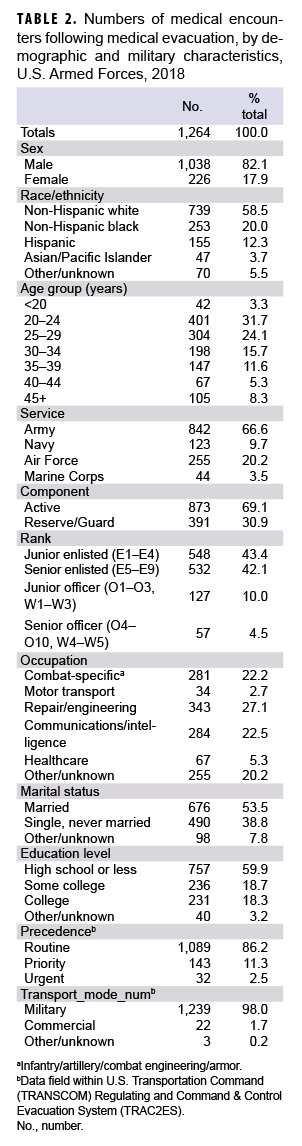
Within the various demographic and military characteristics of those service members who were evacuated, the largest numbers and proportions of evacuees were among non-Hispanic white service members, those aged 20–24 years, members of the Army, junior and senior enlisted personnel, and those in repair/engineering occupations (Table 2).
Most medical evacuations (86.2%) were characterized as having routine precedence. The remainder had priority (11.3%) or urgent (2.5%) precedence. All but 25 (2.0%) of the medical evacuations were accomplished through military transport (Table 2).
Most Frequent Specific Diagnoses
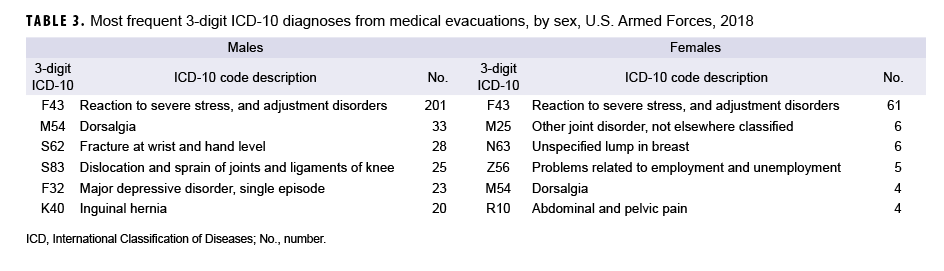
Among both males and females in 2018, "reaction to severe stress, and adjustment disorders" was the most frequent specific diagnosis (3-digit ICD-10 diagnosis code: F43) during initial medical encounters after evacuations (Table 3). The remaining 5 most common 3-digit diagnoses associated with evacuations of males were musculoskeletal disorders ("dorsalgia"), injuries ("fracture at wrist and hand level" and "dislocation and sprain of joints and ligaments of knee"), mental health disorders ("major depressive disorder, single episode"), and digestive system diseases ("inguinal hernia") (Table 3).
Of the top 6 diagnoses most frequently associated with evacuations of female service members, 1 was a mental health disorder ("reaction to severe stress, and adjustment disorders"); 1 was a condition that primarily affects women ("unspecified lump in breast"); 2 were musculoskeletal disorders ("other joint disorder, not elsewhere classified" and "dorsalgia"); 1 was a sign, symptom, and ill-defined condition ("abdominal and pelvic pain"); and 1 was a potential health hazard related to socioeconomic and psychosocial circumstances ("problems related to employment and unemployment") (Table 3).
Disposition
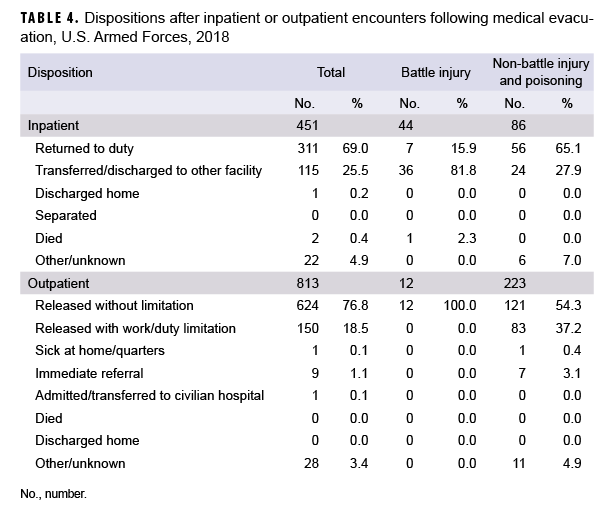
Of the 1,264 medical evacuations reported in 2018, a total of 451 (35.7%) resulted in inpatient encounters. More than two-thirds (69.0%) of all service members who were hospitalized after medical evacuations were discharged back to duty. About one-quarter (25.5%) of service members who were hospitalized after medical evacuations were transferred or discharged to other facilities (Table 4).
Return to duty dispositions were much more likely after hospitalizations for nonbattle injuries (65.1%) than for battle injuries (15.9%). The majority (81.8%) of battle injury-related hospitalizations and a little more than one-quarter (27.9%) of non-battle injury-related hospitalizations resulted in transfers/discharges to other facilities (Table 4).
Slightly more than two-thirds (n=813; 64.3%) of all medical evacuations reported resulted in outpatient encounters only. Of the service members who were treated exclusively in outpatient settings after evacuations, the majority (76.8%) were discharged back to duty without work/duty limitations, 18.5% were released with work/duty limitations, and less than 1% each were admitted/transferred to a civilian hospital, immediately referred, or discharged to "home sick" for recuperation. Service members treated as outpatients after battle injury-related evacuations were more likely to be released without limitations (n=12; 100.0%) than medical evacuees treated as outpatients for non-battle injuries (n=121; 54.3%) (Table 4).
Editorial Comment
This report documented that only 4.4% of all medical evacuations during 2018 were associated with battle injuries. Counts of evacuations for battle injuries were considerably lower (55.6%) in 2018 than in 2014, which is likely a reflection of both the reduction in troop levels that took place during this period and the change in mission away from direct combat. Most evacuations in 2018 were attributed to mental health disorders, followed by non-battle injuries and poisonings; signs, symptoms, and ill-defined conditions; musculoskeletal disorders; and digestive system disorders. Evacuations during the 5-year surveillance period followed a similar but slightly different pattern, with mental health disorders being the most frequent, followed by non-battle injuries, musculoskeletal disorders, signs and symptoms, and digestive system syndromes. Of the major diagnostic categories for which there was more than 1 medical evacuation for both men and women, only percentages of evacuations for injuries (battle and non-battle) and musculoskeletal disorders were noticeably higher among males compared to females. As in previous years, the majority of service members who were evacuated were returned to normal duty status following their post-evacuation hospitalizations or outpatient encounters. However, only about one-third of those evacuated for battle injuries were returned to duty immediately after their initial health care encounters.
Overall, the changes in numbers of medical evacuations over the course of the surveillance period reflect the drawdown of U.S. troops from Afghanistan leading up to the end of OEF.9 As OFS began, U.S. troop withdrawal slowed and began to level off in 2015.9 The relatively low percentage of medical evacuations in 2018 suggests that most deployers were sufficiently healthy and ready for their deployments and received the medical care in theater necessary to complete their assignments without having to be evacuated. Moreover, the fact that very few medical evacuations were conducted for chronic conditions such as hematologic disorders and congenital anomalies supports the idea that most deployers were sufficiently healthy for deployment. However, deployed service members are not immune to such conditions. For example, there was 1 medical evacuation for congenital anomalies in 2018 that was due to an arteriovenous malformation of cerebral vessels (data not shown). Because congenital anomalies may not be identified and diagnosed until later in life,10 such diagnoses should not be ruled out.
The proportion of medical evacuations attributed to mental health disorders (28.2%) was slightly higher than the proportion reported in a recent MSMR analysis of medical evacuations in 2017 (23.6%)5 but considerably higher than the proportion (11.6%) reported in an earlier MSMR report examining evacuations from Iraq during a 9-year period between 2003 and 2011.1 However, that article also reported that during the last 4 years of the surveillance period (2008–2011), as the proportion of evacuations for battle injuries fell sharply, the proportions of evacuations for mental disorders increased dramatically for both males (peak of 20.9% in 2010) and females (peak of 26.6% in 2010). Although some studies have indicated improved access to mental health care in deployed settings, the results from the current analysis indicate that mental health diagnoses still represent the single most common basis for medical evacuations out of the CENTCOM AOR.11 This could be due, at least in part, to variations in the availability of mental health care in deployed settings. In these settings, the distribution of providers and clinics that deliver such services is uneven and varies according to factors such as the number of deployed personnel and the assessed needs of the particular unit.11 It is also likely that some service members with mental health diagnoses may be evacuated because their estimated recovery times are too long. In addition, although the number of mental health care providers in Afghanistan increased from 2005 through 2010, this number decreased after 2013 as part of the overall drawdown of U.S. troops from the region.11
Several important limitations should be considered when interpreting the results of this analysis. Because deployment data are no longer available in the DMSS, rates of medical evacuations per deployed person-time were not able to be calculated, precluding comparisons with recent MSMR analyses. In addition, direct comparisons of numbers and percentages of medical evacuations by cause, as between males and females, can be misleading; for example, such comparisons do not account for differences between the groups in other characteristics (e.g., age, grade, military occupation, locations, and activities while deployed) that are significant determinants of medical evacuation risk. Moreover, because data about the characteristics of the entire deployed population of service members were not available, it was not possible to determine if the members of demographic and military groups listed above were over- or underrepresented among the evacuees. Also, for this report, most causes of medical evacuations were estimated from primary (first-listed) diagnoses that were recorded during hospitalizations or initial outpatient encounters after evacuation. In some cases, clinical evaluations in fixed medical treatment facilities after medical evacuations may have ruled out serious conditions that were clinically suspected in the theater. For this analysis, the causes of such evacuations reflect diagnoses that were determined after evaluations outside of the theater rather than diagnoses—perhaps of severe disease—that were clinically suspected in the theater. To the extent that this occurred, the causes of some medical evacuations may seem surprisingly minor.
Overall, the results highlight the continued need to tailor force health protection policies, training, supplies, equipment, and practices based on characteristics of the deployed force (e.g., combat vs. support; male vs. female) and the nature of the military operations (e.g., combat vs. humanitarian assistance).
References
- Armed Forces Health Surveillance Center. Medical evacuations from Operation Iraqi Freedom/Operation New Dawn, active and reserve components, U.S. Armed Forces, 2003–2011. MSMR. 2012;19(2):18–21.
- Armed Forces Health Surveillance Center. Surveillance snapshot: Medical evacuations from Operation Enduring Freedom (OEF), active and reserve components, U.S. Armed Forces, Oct. 2001–Dec. 2011. MSMR. 2012;19(2):22.
- Armed Forces Health Surveillance Center. Medical evacuations from Afghanistan during Operation Enduring Freedom, active and reserve components, U.S. Armed Forces, Oct. 7, 2001–Dec. 31, 2012. MSMR. 2013;20(6):2–8.
- Armed Forces Health Surveillance Branch. Medical evacuations, active and reserve components, U.S. Armed Forces, 2013–2015. MSMR. 2017;24(2):15–21.
- Armed Forces Health Surveillance Branch. Update: Medical evacuations, active and reserve components, U.S. Armed Forces, 2017. MSMR. 2018;25(7):17–22.
- Garamone J. Dunford: U.S. Forces busy implementing defense strategy worldwide. DOD News. 28 Aug. 2018. https://dod.defense.gov/News/Article/Article/1614521/dunford-us-forces-busy-implementing-defense-strategy-worldwide/. Accessed March 11, 2019.
- Lead Inspector General for Overseas Contingency Operations. Operation Freedom's Sentinel: Report to the United States Congress.https://media.defense.gov/2018/May/21/2001919976/-1/-1/1/FY2018_LIG_OCO_OFS2_MAR2018_3.PDF. Accessed March 11, 2019.
- North Atlantic Treaty Organization. Resolute Support Mission (RSM): key facts and figures. https://www.nato.int/nato_static_fl2014/assets/pdf/pdf_2018_06/20180608_2018-06-RSM-placemat.pdf. Accessed March 11, 2019.
- Defense Manpower Data Center. DOD personnel, workforce reports and publications.https://www.dmdc.osd.mil/appj/dwp/dwp_reports.jsp. Accessed March 12, 2019.
- The Centers for Medicare and Medicaid Services and the National Center for Health Statistics. ICD-10-CM Official Guidelines for Coding and Reporting. FY 2018.https://www.cms.gov/Medicare/Coding/ICD10/Downloads/2018-ICD-10-CM-Coding-Guidelines.pdf. Accessed March 12, 2019.
- United States Government Accountability Office. Report to Congressional Committees. Defense health care: DOD is meeting most mental health care access standards, but it needs a standard for follow-up appointments. April 2016. https://www.gao.gov/assets/680/676851.pdf. Accessed March 12, 2019.