Abstract
SARS-CoV-2 ICD-10-CM-based case definitions are lacking in the literature. This analysis was conducted to evaluate the performance metrics of 3 COVID-19 case definitions among Department of Defense (DOD) beneficiaries. SARS-CoV-2 tested specimens collected from 1 March 2020 to 28 February 2021 were matched to ambulatory medical encounters (68% match). The COVID-19 case definition (ICD-10-CM: U07.1) had high specificity (99%) and positive predictive value (PPV) (94%) but low to moderate (29%–66%) sensitivity. The COVID-specific case definition (10 additional codes added), had moderate to high specificity (82–93%), moderate sensitivity (65–75%), and low to moderate PPV (23%–77%). The COVID-like illness case definition (19 additional codes added to the COVID-specific definition), had moderate specificity (65%–86%), moderate sensitivity (76%–79%), and low to moderate PPV (15%–62%). Regardless of the case definition, all metrics improved over the surveillance period. The COVID-19 case definition is ideal for studies that need to ensure all cases are true positives. However, for broad surveillance efforts, the COVID-specific case definition may be the best to maximize specificity without a large decrease in sensitivity and PPV.
What are the new findings?
This is the first evaluation of ICD-10-CM-based cased definitions for COVID-19 surveillance among DOD health care beneficiaries. The 3 case definitions ranged from highly specific to a lower specificity, but improved balance between sensitivity and specificity.
What is the impact on readiness and force health protection?
The development and use of these ICD-10-CM case definitions should improve the DOD’s ability to provide comprehensive population level COVID-19 surveillance and will allow the DOD to better assess the spread and impact of COVID-19 among military beneficiaries.
Background
The emergence of SARS-CoV-2 in 2019 and the rapid global spread of the virus throughout 2020 and 2021 required quick implementation and development of clinical, laboratory, and epidemiologic surveillance efforts to identify, track, and mitigate the virus. Prior to 1 April 2020, ICD-10-CM coding guidance for SARS-CoV-2 associated medical encounters was not available. In April of 2020, the Centers for Disease Control and Prevention (CDC) released official ICD-10-CM coding and reporting guidelines for use in the U.S. for a confirmed diagnosis of COVID-19.1 However, a report on the early use of U07.1 within the DOD, found that 30% of the encounters evaluated did not meet the criteria for COVID-19 and incorrectly documented encounters for recruit screening for COVID-19 as opposed to an actual infection.2 However, the report also found a lack of full capture of laboratory results within the DOD, which warrants consideration of alternative methods of case identification, such as validated standardized ICD-10-CM case definitions. A review of the current literature found a paucity of data on administrative case definitions for COVID-19, with most publications evaluating case definitions using symptom reporting as opposed to ICD-10-CM coding or studies focusing solely on U07.1.3–8 Therefore, to enhance the DOD’s ability to conduct COVID-19 surveillance among the military population as a whole, this study was conducted to evaluate 3 ICD-10-CM-based case definitions for COVID-19 and COVID-like illnesses for ambulatory encounters.
Methods
The study population consisted of all DOD health care beneficiaries who had a specimen collected between 1 March 2020 and 28 February 2021 for SARS-CoV-2 laboratory testing. Standardized laboratory data were provided by the Navy and Marine Corps Public Health Center (NMCPHC). Only laboratory tests reported through the Composite Health Care System (CHCS) or MHS GENESIS were captured in the study. Eligible SARS-CoV-2 laboratory tests included both polymerase chain reaction (PCR) and antigen tests. The analysis allowed for 1 specimen per day per individual, preferentially selecting a specimen with a positive result over a negative result over an unknown result.
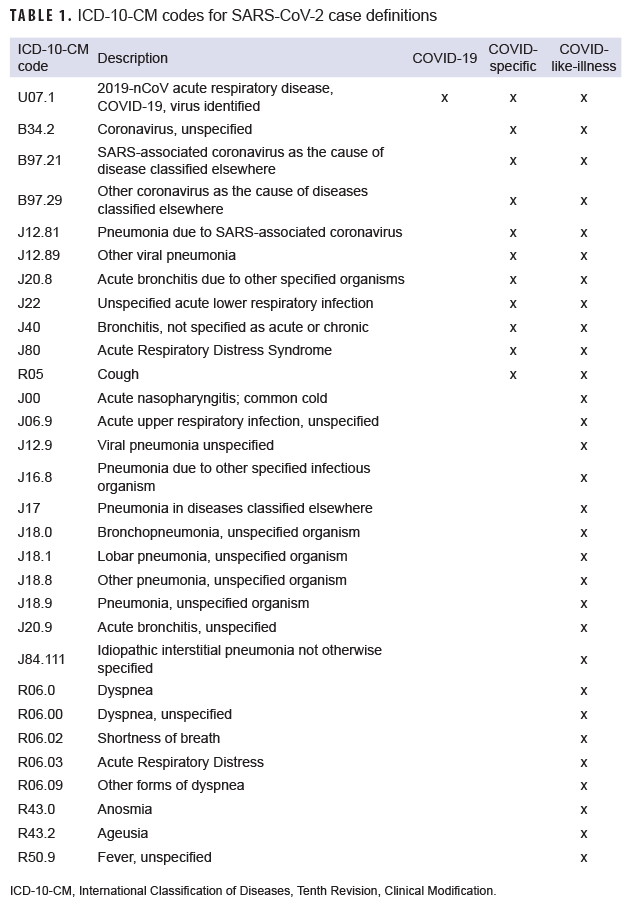
Data from the Defense Medical Surveillance System (DMSS) were used to match each laboratory test to a single ambulatory medical encounter occurring within 7 days before or after the tested specimen collection date.9 If more than 1 encounter was temporally associated with a laboratory test, the priority for selection was given to encounters with a COVID-19 diagnostic code, COVID-specific diagnostic code, a COVID-like illness (CLI) diagnostic code, and then any other encounter (Table 1). Laboratory tests without a matching encounter were excluded from the sensitivity/specificity analysis.
The surveillance period was partitioned into 4 separate periods for the analysis: 1 March 2020–31 May 2020, 1 June 2020–31 August 2020, 1 September 2020–30 November 2020, and 1 December 2020–28 February 2021. This partitioning was done to account for changing availability of ICD-10 codes and coding practices over the course of the first year of the COVID-19 pandemic. For each period, the percentage of laboratory tests that matched to any medical encounter was calculated. Three COVID-19 case definitions were evaluated in the analysis; COVID-19, COVID-specific, and CLI case definitions (Table 1). The case definitions were not mutually exclusive, but rather expanded upon the prior case definition. The case definitions were developed early in the pandemic by Armed Forces Health Surveillance Division (AFHSD) physicians and epidemiologists using interim clinical case definitions proposed by the CDC and expert knowledge, which incorporated random chart reviews of cases to better ascertain coding practices of DOD physicians.1 The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for each case definition and time period (Table 2).
Results
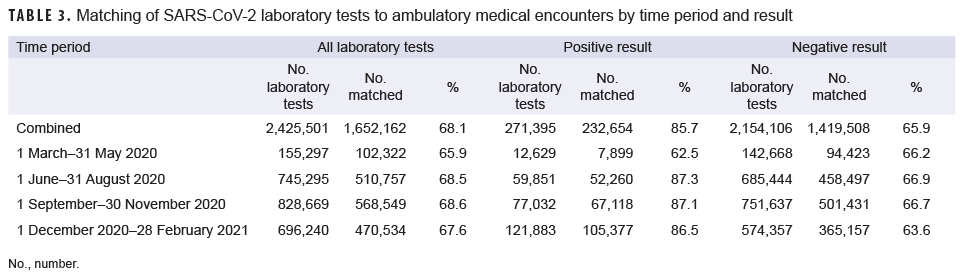
A total of 2,425,501 SARS-CoV-2 laboratory tests were identified for the entire study period. The lowest number of tests were conducted in the March–May 2020 time period (155,297 tests) and the highest number were conducted in the September–November 2020 time period (828,669 tests) (Table 3). Overall, 68.1% of laboratory tests were matched to medical encounters. A higher percentage of positive laboratory tests (85.7%) were matched to ambulatory medical encounters than negative laboratory tests (65.9%). The percentages of laboratory tests that matched to medical encounters were relatively similar across time periods, with the exception of positive laboratory tests, for which only 62.5% matched to encounters in the first time period, while about 87% matched to encounters in the 3 later time periods.
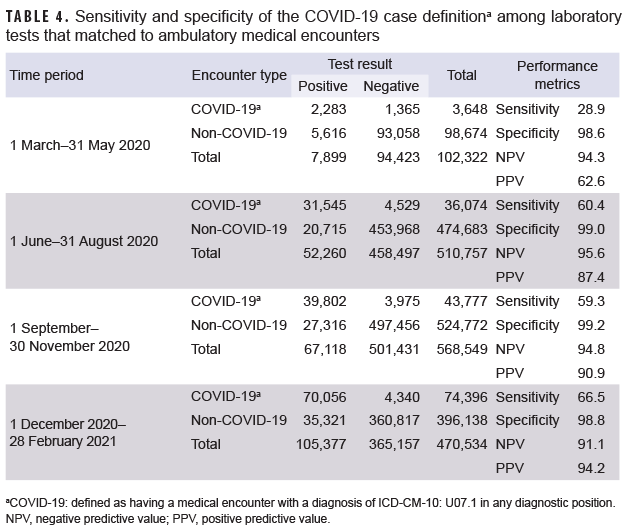
Among laboratory tests that matched to medical encounters, the 3 COVID-19 case definitions were evaluated for sensitivity, specificity, PPV and NPV during each of the 4 time periods. NPV was high regardless of the time period or case definition (Tables 4–6). As expected, the COVID-19 case definition had very high specificity (98.6%–99.2%) regardless of the time period. However, the sensitivity of this case definition ranged from low (28.9%) in March–May 2020 to moderate (66.5%) in December–February 2021 (Table 4). The PPV of the COVID-19 case definition also increased through the first year of the pandemic; from 62.6% during the first period to 94.2% during the last period evaluated.
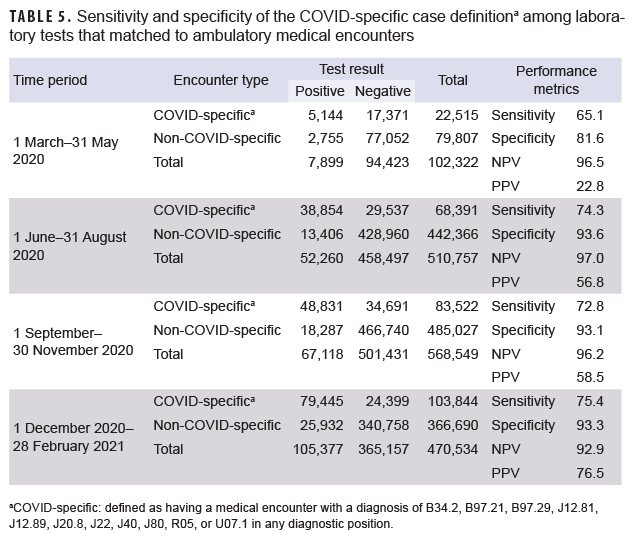
The sensitivity, specificity, and PPV of the COVID-specific case definition all increased over time (Table 5). The sensitivity of this case definition was moderate during the first period (65.1%) and increased to moderately high (75.4%) during the last period. The specificity was moderately high during the first period (81.6%) and increased to be high (93.3%) during the last period. The PPV of this case definition was very poor (22.8%) early in the pandemic, but improved to a moderately high level (76.5%) during the last period of surveillance.
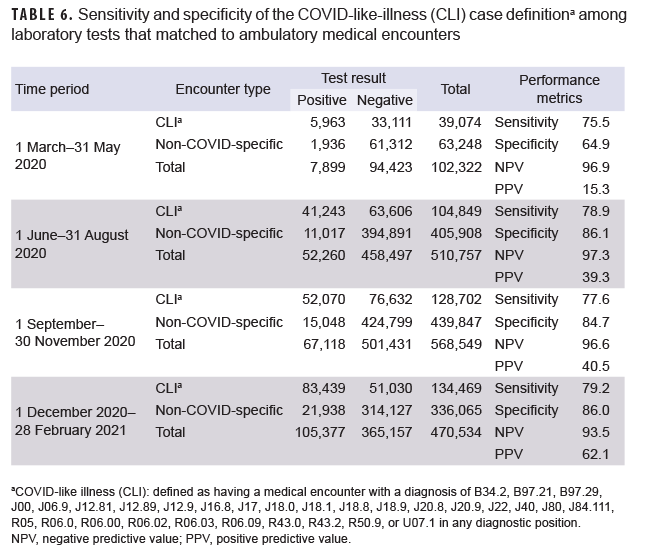
The broadest of the 3 case definitions, CLI, had the highest sensitivity (range=75.5%–79.2%) compared to the other case definitions, but it was only slightly higher than the COVID-specific case definition (Table 6). As expected, specificity was lowest among the CLI case definition compared to the other case definitions. The specificity of this case definition ranged from 64.9% during the first period to 86.0% during the last period. The PPV was very low during the first period (15.3%), but increased to a moderate level (62.1%) by the last period of surveillance.
Editorial Comment
As the COVID-19 pandemic expanded in the U.S. in March 2020, surveillance, diagnosis, and tracking efforts were rapidly deployed and evolved. With the addition of new ICD-10-CM codes for COVID-19 and guidance for their use, it was crucial to develop and evaluate various ICD-10-CM based case definitions to allow for accurate, population-level surveillance of COVID-19. This study evaluated 3 COVID-19 case definitions to determine and compare their sensitivity, specificity, and PPV.
Two-thirds of laboratory tests could be matched to ambulatory encounters. Given that there were multiple locations where individuals could be tested for the SARSCoV-2 virus (e.g., medical offices, pharmacies, drive-thru testing locations), many of which would not be linked to an ambulatory medical encounter, this finding is not surprising. However, positive laboratory tests were more likely to have an associated ambulatory encounter than negative tests. This finding indicates that individuals who tested positive may have symptoms requiring medical treatment or consultation with a medical provider.
Results were as expected, with the highest specificity and PPV occurring with the most specific case definition of U07.1. The CDC issued official coding and reporting guidelines to use this code for a confirmed diagnosis of COVID-19.1 The timing of this release, 1 April 2020, aligns with the finding of lower sensitivity and PPV of this code during the March–May 2020 period, when this code may not have been available to all providers and/or training on its use was being rolled out. One study found that it took 2 weeks for U07.1 to be widely used for COVID-19 hospitalizations in the U.S.6 The PPV of U07.1 for the entire study period, 91.0%, was higher than a previous publication among Veterans Affairs outpatient encounters, which reported PPV to be 77.7% during a similar time period.7 Although published studies on the sensitivity and specificity of U07.1 among ambulatory encounters were not available at the time of this report, there have been 2 publications among hospitalizations: 1 among adults and 1 among a pediatric population.6,8 All studies found high specificity of the code (current study: 98.9%, adult study: 99.0%, pediatric study: 99.9%). However, the hospitalization studies found much higher sensitivity of U07.1 (adult study: 98.0%; pediatric study: 89.7%) compared to the current ambulatory encounter sensitivity (66.5% during the last period). This difference may be due to the fact that inpatient encounters require a nosologist (an individual who specializes in the systemic classification of diseases) to generate the discharge diagnoses, whereas this is not necessarily done with ambulatory encounters. Additionally, medical providers may not have laboratory test results available when generating ambulatory encounter diagnostic codes and therefore may have been hesitant to code U07.1 without laboratory confirmation.
With the addition of more ICD-10-CM codes for the COVID-specific and CLI case definitions, sensitivity increased, but at the expense of specificity and PPV. These case definitions provided a better balance between sensitivity and specificity compared to standardized case definitions used for other respiratory infections, such as influenza-like illness, which had very high sensitivity (92–93%), but very low specificity (26–30%).10 However, none of the COVID-19 case definitions reached a sensitivity as high as the influenza-like-illness definitions. This may be due to a larger variety of ICD-10 codes being used by providers, especially early in the pandemic, and the more diverse symptoms associated with COVID-19 cases compared to influenza cases.11–13
This analysis was limited to medical encounters for which SARS-CoV-2 tests were ordered at military treatment facilities. As multiple SARS-CoV-2 testing locations were available, separate from MTFs, there is the possibility that the study population was not representative of DoD beneficiaries tested for SARS-CoV-2 during this time period. Additionally, the analysis required a medical encounter, so asymptomatic and non-medically attended individuals will not be captured in this analysis and should be considered a gap in surveillance utilizing ICD-10-CM case definitions. However, with those limitations, this analysis was able to provide data on a population level that can be used to enhance public health surveillance of COVID-19 cases. Improved surveillance for COVID-19 can provide a more accurate assessment of the burden of disease and the impact on military readiness among service members. As with all surveillance efforts, decisions on the most appropriate case definition to use need to incorporate an understanding of the data sources being used, the population being studied, and the purpose of the surveillance.
Author affiliations: Defense Health Agency, Armed Forces Health Surveillance Division, Silver Spring, MD (Dr. Eick-Cost, Ms. Fedgo).
References
1. Centers for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19) 2020 interim case definition, Approved April 5, 2020. Accessed 19 Jan 2022. https://ndc.services.cdc.gov/case-definitions/coronavirus-disease-2019-2020
2. Clausen S, Stahlman S, Cost A. Early use of ICD-10-CM code “U07.1, COVID-19” to identify 2019 novel coronavirus cases in Military Health System administrative data. MSMR. 2000;27(05):55–59.
3. Pulia MS, Hekman DJ, Glazer JM, et al. Electronic health record-based surveillance for community transmitted COVID-19 in the emergency department. West J Emerg Med. 2020;21(4):748–751.
4. Crabb BT, Lyons A, Bale M, et al. Comparison of International Classification of Diseases and related health problems, tenth revision codes with electronic medical records among patients with symptoms of coronavirus disease 2019. JAMA Netw Open. 2020;3(8):e2017703.
5. Kluberg SA, Hou L, Dutcher SK, et al. Validation of diagnosis codes to identify hospitalized COVID-19 patients in health care claims data [published online ahead of print, 2021 Dec 16]. Pharmacoepidemiol Drug Saf. 2021;10.1002/pds.5401.
6. Kadri SS, Gundrum J, Warner S, et al. Uptake and accuracy of the diagnosis code for COVID-19 among US hospitalizations. JAMA. 2020;324(24):2553–2554.
7. Lynch KE, Viernes B, Gatsby E, et al. Positive predictive value of COVID-19 ICD-10 diagnosis codes across calendar time and clinical setting. Clin Epidemiol. 2021;13:1011–1018.
8. Blatz AM, David MZ, Otto WR, Luan X, Gerber JS. Validation of International Classification of Disease-10 code for identifying children hospitalized with coronavirus disease-2019. J Pediatric Infect Dis Soc. 2021;10(4):547–548.
9. Rubertone MV, Brundage JF. The Defense Medical Surveillance System and the Department of Defense serum repository: glimpses of the future of public health surveillance. Am J Public Health. 2002;92(12):1900–1904.
10. Eick-Cost AA, Hunt DJ. Assessment of ICD-9-based case definitions for influenza-like illness surveillance. MSMR. 2015;22(9):2–7.
11. Mayo Clinic. Unusual coronovirus (COVID-19) symptoms: What are they? Accessed 26 Jan 2022. https://www.mayoclinic.org/diseases-conditions/coronavirus/expert-answers/coronavirus-unusualsymptoms/faq-20487367
12. Centers for Disease Control and Prevention. Symptoms of COVID-19. Accessed 26 Jan 2022. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html
13. Burke RM, Killerby ME, Newton S, et al. Symptom profiles of a convenience sample of patients with COVID-19 - United States, January-April 2020. MMWR Morb Mortal Wkly Rep. 2020;69(28):904–908.