This study compared estimates of the prevalence of and risk factors for tobacco and nicotine use obtained from the 2018 Health Related Behaviors Survey and Periodic Health Assessment survey. The HRBS and the PHA are important Department of Defense sources of data on health behavior collected from U.S. military service members. While their collection methods differ, some survey questions are similar, which provides an opportunity to compare survey estimates. Active duty service members consistently reported a much lower prevalence of all types of tobacco and nicotine use on the PHA compared to the HRBS: cigarettes (11.1% vs. 18.4%), e-cigarettes (7.3% vs. 16.2%), chewing tobacco (9.7% vs. 13.4%), any tobacco or nicotine use (25.3% vs. 37.8%), and use of two or more tobacco or nicotine products (5.8% vs. 17.4%). Associations between tobacco and nicotine use as well as demographic and other behavioral variables were fairly similar, including age, sex, education, race and ethnicity, rank, and alcohol use. The associations with service branch, body mass index, and sleep were inconsistent. This results of this study suggest that the PHA can provide timely information on trends in military tobacco and nicotine use over time, but much higher estimates from the confidential, voluntary HRBS reported in this study suggest that the command-directed PHA may substantially underestimate the prevalence of all types of tobacco and nicotine use.
What are the new findings?
U.S. service members consistently reported much lower prevalence of use of tobacco and nicotine on the PHA compared to the HRBS. The command-directed PHA may provide timely information on trends and risk factors for tobacco and nicotine use but substantially underestimates their use.
What is the impact on readiness and force health protection?
The use of tobacco and nicotine remains an important threat to the health and readiness of U.S. military service members. Both the HRBS and the PHA provide unique and valuable information for military policy guidance on force health protection and readiness, and they should be used in tandem.
Background
The HRBS is a confidential, cross-sectional survey sponsored by the Department of Defense for better understanding of the health behaviors of all military branches. The HRBS was most recently conducted in 2018 by the RAND Corporation (Santa Monica, CA). Despite its utility in monitoring health-related behaviors in the U.S. military over time, the HRBS is limited by a low response rate, increasing the probability of bias.1
The periodic health assessment is an annual, standardized health assessment throughout the military services to “assess currency of individual medical readiness requirements,” in accordance with DOD Instructions 6025.19 and 6200.06.2,3 The PHA collects some survey items similar to the HRBS, including questions on smoking and tobacco and nicotine product use.3 As the PHA must be reviewed by a health care provider, often in a direct, personal encounter,3 its data may not be reported accurately due to service member concerns about negative career consequences, or other social desirability misclassification biases.4
In 2015 the prevalence of cigarette use reported in the HRBS within the active duty population (13.8%) declined for the first time to a point lower than the general U.S. population (15.1%).5-8 In contrast, the prevalence of electronic cigarette (e-cigarette) use—also known as vaping—was higher in the U.S. military (12.4%) than in the general U.S. population (3.5%).5,9 Particularly notable was the much higher prevalence of e-cigarette use among the 17-24 year old age group in the military (22.8%) compared to the general population (5.2%). The most recently published HRBS results from 2018 indicate substantial increases in overall cigarette use (18.4%) and e-cigarette use (16.2%) compared to 2015.1
A comparison of these two data sources could be helpful in determining the validity and utility of both data sources both for surveillance purposes and public health guidance. Furthermore, such a comparison could obviate the need for questions in the HRBS that are already covered in the PHA, if the two data sources are found to provide similar information.1 This study compares estimates of prevalence and risk factors for tobacco and nicotine use among active duty U.S. service members that were self-reported in 2018 in the HRBS and the PHA.
Methods
The 2018 HRBS study design included population-based stratified random sampling and non-responsive weights, which were utilized to make the analytic sample obtained from the study representative of the eligible service member population.1 Publicly available data from the 2018 HRBS, the most recent data released, were utilized to create a sampling frame of 1,357,219 active component service members, which was segmented into 50 strata, based on the interaction of service branch (five categories), pay grade (five categories), and sex. Of 199,996 invited eligible active duty service members, 17,166 responded to the survey request, with an overall weighted response rate of 9.6%.1 Sampling weights by post-stratification were used to represent the population. The low response rate of HRBS increases risk of selection bias and bias due to unobserved data. To increase representativeness, HRBS used SAS 9.4 to produce summary statistics, with confidence interval estimates computed using the Wald method.1 Missing data among respondents was addressed via imputation methods such as predictive mean matching to impute binary, ordinal, and continuous variables, and polytomous regression to impute categorical data.1
All PHAs completed (n=854,579) during calendar year 2018 by ACSMs in the Army, Navy, Air Force, Marine Corps, and Coast Guard were queried from the Defense Medical Surveillance System (DMSS).
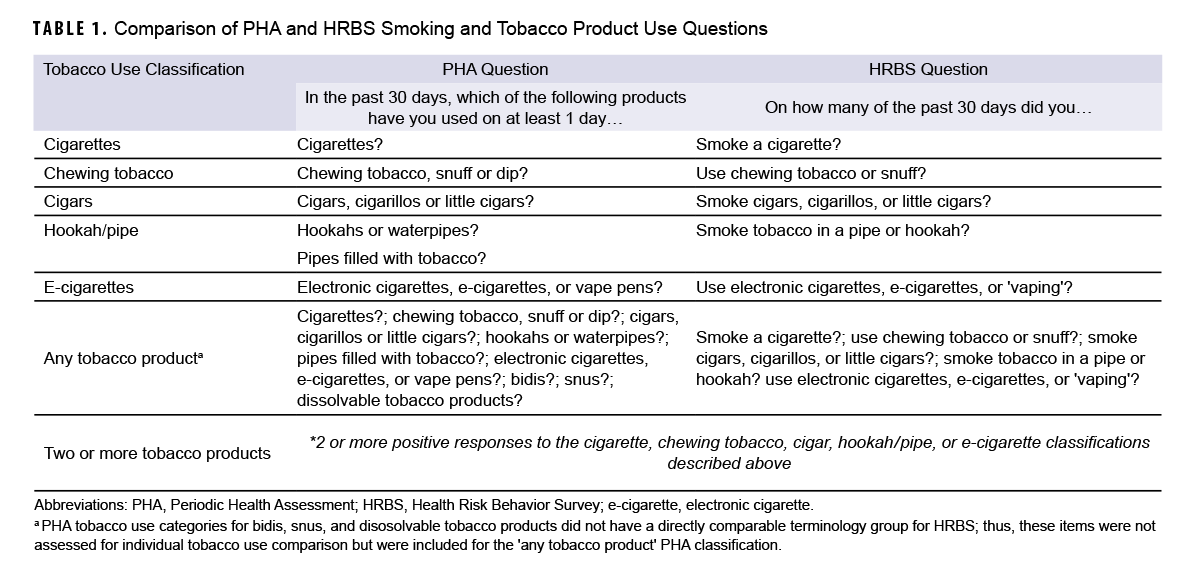
HRBS and PHA questions assessing tobacco and nicotine use, demographic characteristics, and other exposures were reviewed. The questions that assessed tobacco and nicotine use were very similar, as shown in Table 1. Tobacco and nicotine use outcomes were assessed for five types of single product use within the past 30 days: cigarettes, chewing tobacco or snuff, cigars (cigars, cigarillos, or little cigars), tobacco use in a pipe or hookah, and electronic cigarettes (‘e-cigarettes’ or ‘vaping’). The use of any tobacco or nicotine product use and two or more forms of any single tobacco or nicotine product use were also assessed.
In both surveys, demographic information (age, sex, race and ethnicity, branch of service, rank, education); body mass index; and health-related behaviors such as sleep (average hours of sleep in a 24-hour period over the last 30 days) and alcohol use (usual number of drinks containing alcohol on day[s] the service member drank in the last 30 days) were collected similarly. The assessment of sexually-transmitted infection risk defined by the HRBS included self-reporting of an STI (such as gonorrhea, syphilis, chlamydia, HPV, or genital herpes) within the past year. In contrast, the PHA defined STI risk by one or more of the following: a new sex partner in the past three months; more than one sex partner in the last 12 months; sexually active women less than 25 years of age; inconsistent use of latex condoms; men who have sex with men; sexual contact with person(s) with known STIs or risk of STI; exchanged money or drugs for sex; or injected drug use.
HRBS estimates were generated using sample weights to generate representative active component population estimates, as previously reported,8 while PHA data were reported using unweighted estimates. Relative frequency analyses were performed to describe the distribution of respondents’ demographics and health behaviors in both surveys. The prevalence estimates of tobacco or nicotine use classification groups were reported. The standard errors and CIs for weighted HRBS estimates were computed using the Taylor series method. Adjusted odds ratios of tobacco or nicotine product use and 95% CIs were calculated using logistic regression, reported separately for the HRBS and PHA; sample weights were again used for HRBS (i.e., weighted logistic regression) but not PHA analysis. Statistical significance was set at 0.05 for all statistical tests. SAS statistical software 9.4 (SAS Institute, Cary, NC) was used in all analyses.
Results
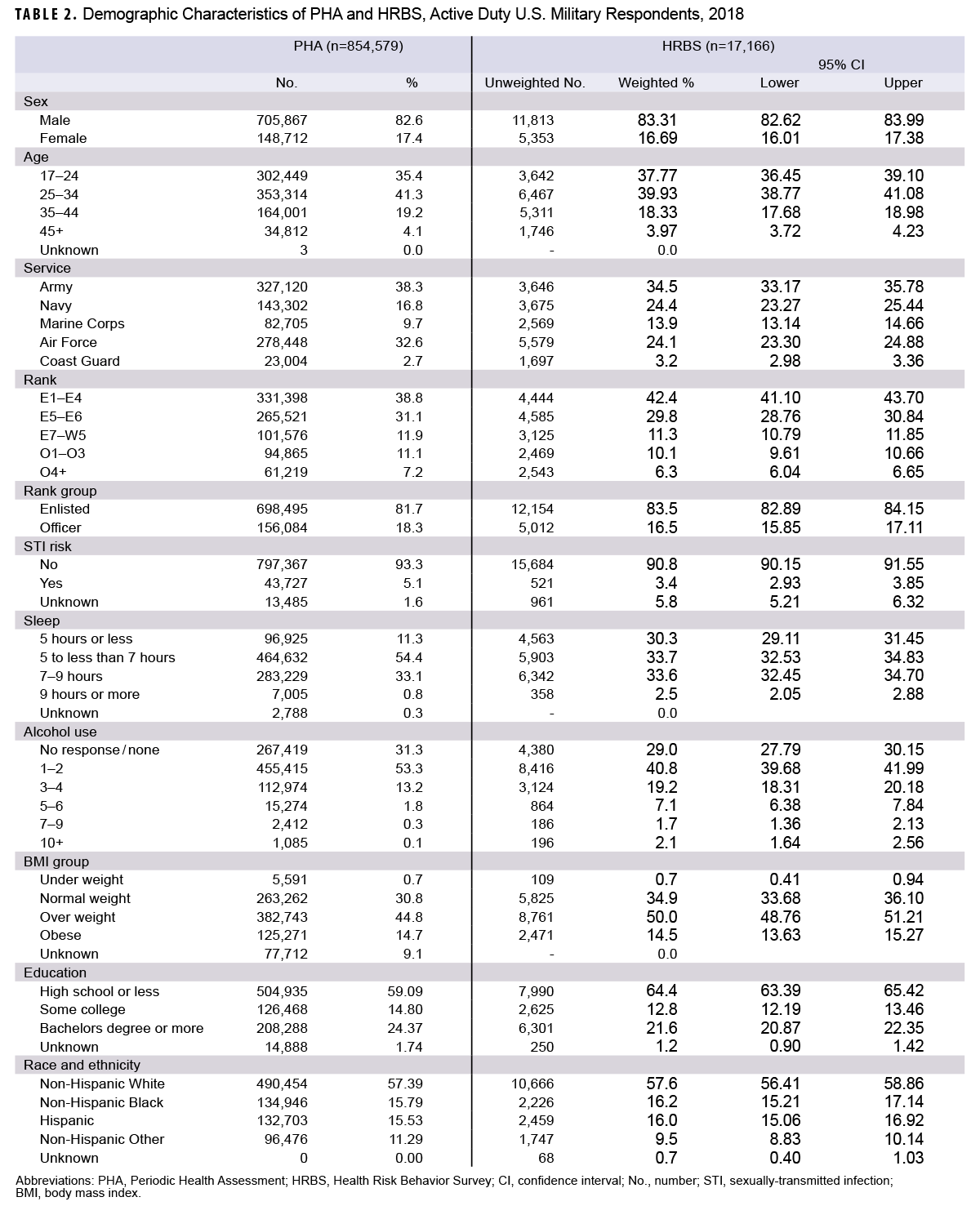
A total of 17,166 (9.6% weighted response among those invited) and 854,579 (64% of the active component population) respondents from the HRBS and the PHA, respectively, were included in the analysis (Table 2). PHA response distributions compared to the HRBS were lower for respondents who were: under age 25; of junior or enlisted ranks; in the Navy or Marine Corps; overweight; and with education levels of high school or less. Notably, compared with PHA respondents, HRBS respondents reported shorter sleep duration (5 hours or less per night: 30.3% vs. 11.3%) and more frequent alcohol use (three or more times per week: 30.2% vs. 15.4%).
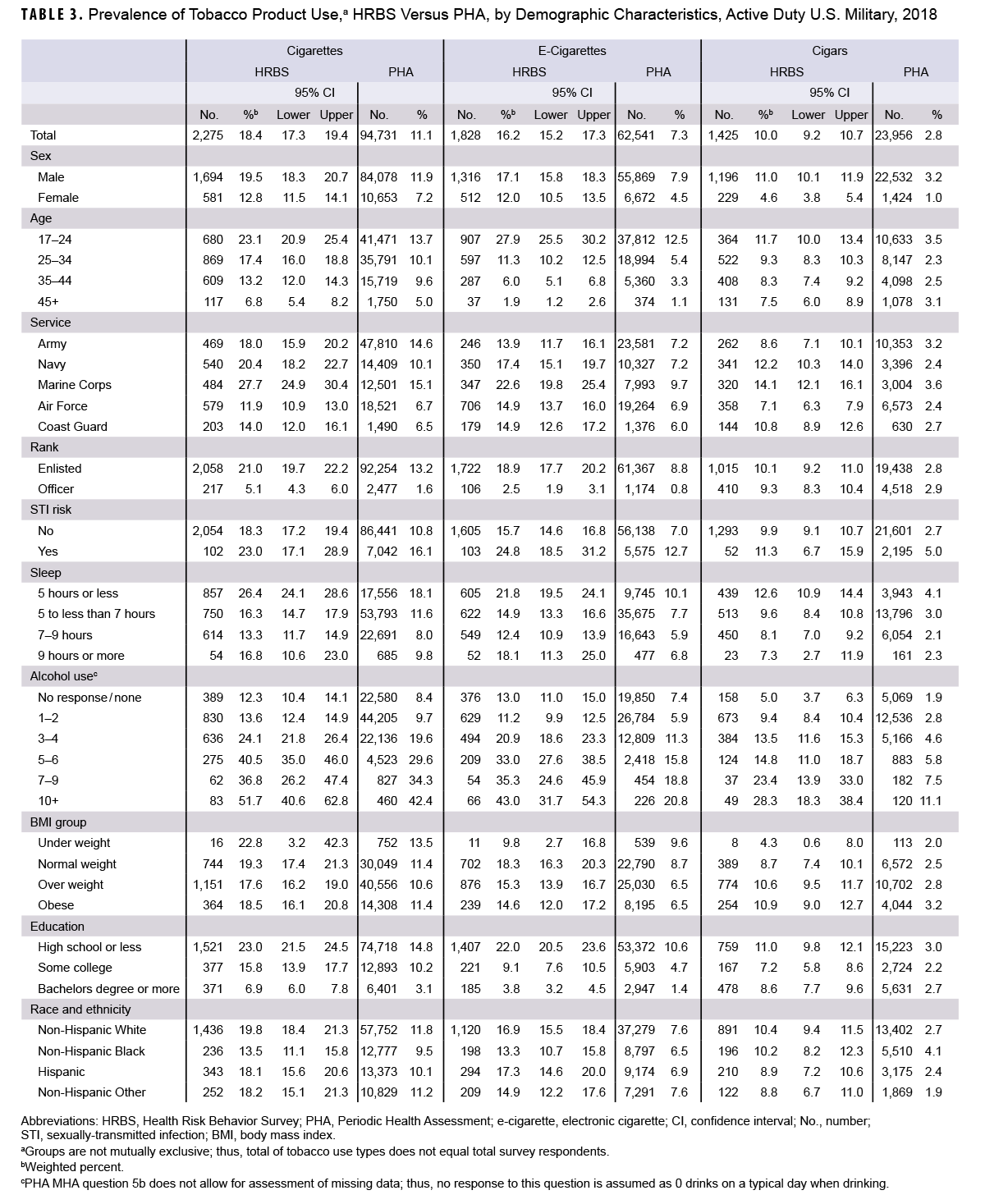
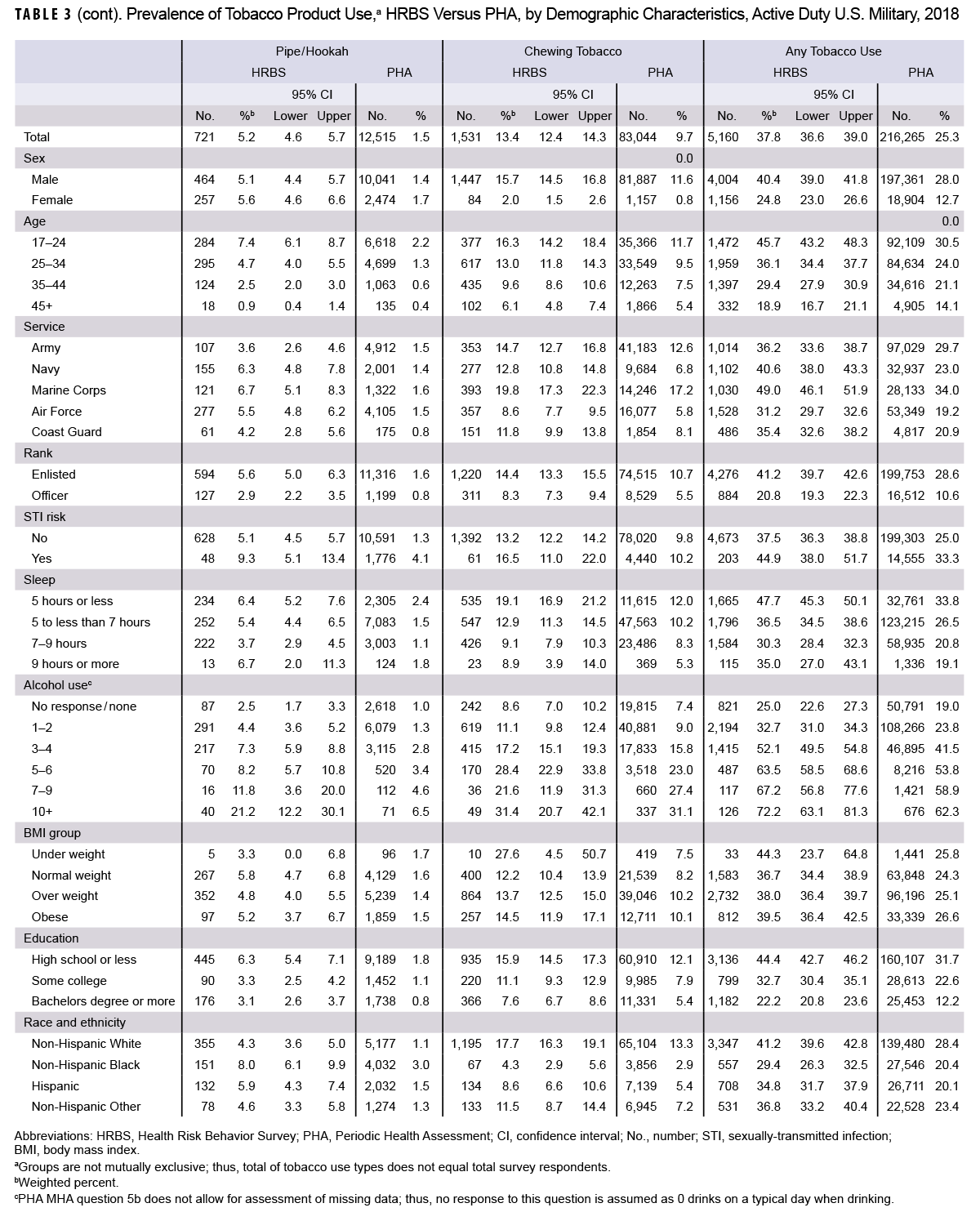
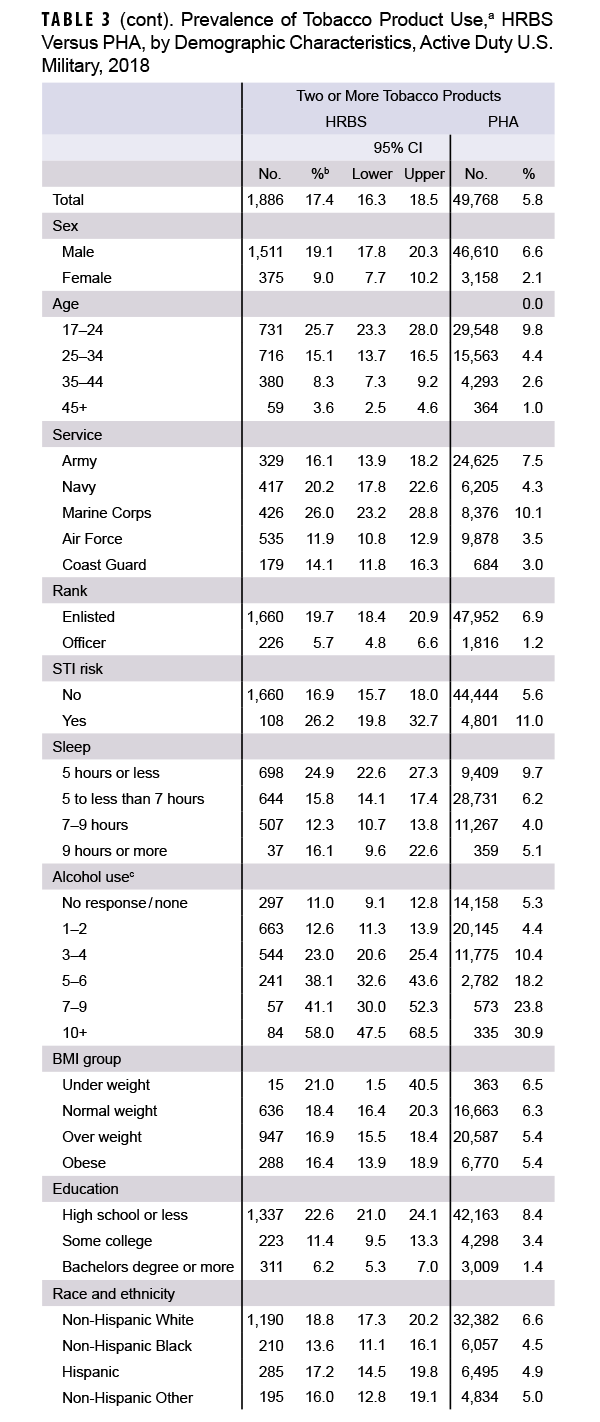
Service members consistently reported a much lower prevalence of all types of tobacco and nicotine use in the PHA than in the HRBS (Table 3), for: cigarettes (11.1% vs. 18.4%), e-cigarettes (7.3% vs. 16.2%), cigars (2.8% vs. 10.0%), pipes or hookahs (1.5% vs. 5.2%), and chewing tobacco (9.7% vs. 13.4%). PHA estimates were also lower for any tobacco or nicotine use (25.3% vs. 37.8%) and use of two or more tobacco or nicotine products (5.8% vs. 17.4%).
Tobacco and nicotine use associations with demographic and behavioral variables were mostly similar between the two data sources. Prevalence for all types of tobacco and nicotine use was highest in youngest service members and decreased with age; of note, prevalence among 17 to 24 year olds was much higher in the HRBS for both cigarette use (23.1% vs. 13.7%) and e-cigarette use (27.9% vs. 12.5%). Prevalence of all types of tobacco or nicotine use was higher among men than women, except for pipe and hookah use, which was higher among women. Service members who were enlisted, at increased STI risk, used more alcohol, or had lower education levels had generally a higher prevalence of all types of tobacco or nicotine use.
Non-Hispanic Black service members had the lowest prevalence of cigarette, e-cigarette, and chewing tobacco use but highest prevalence of pipe or hookah use (8.0%) and high levels of cigar use (10.2%). Hispanic service members had the highest prevalence of e-cigarette (17.3%) use and high levels of cigarette use (18.1%). These findings were generally consistent between the data sources.
Some associations between demographic and behavioral factors and tobacco or nicotine use were inconsistent between the two data sources. Among the services, Marines had the highest use of all types of tobacco or nicotine, but otherwise associations between services varied by type of product used and the data source. For example, prevalence of cigarette use among Navy service members (20.4%) was higher than among Army service members (18.0%) according to HRBS data, but the relationship was reversed for the PHA—estimated prevalence in the Navy (10.1%) was lower than in the Army (14.6%). Associations of hours of sleep per night were also inconsistent with some types of tobacco or nicotine use. Much of the apparent “under-weight” BMI heterogeneity between the two data sources was likely due to the small numbers of HRBS respondents, leading to unstable estimates.
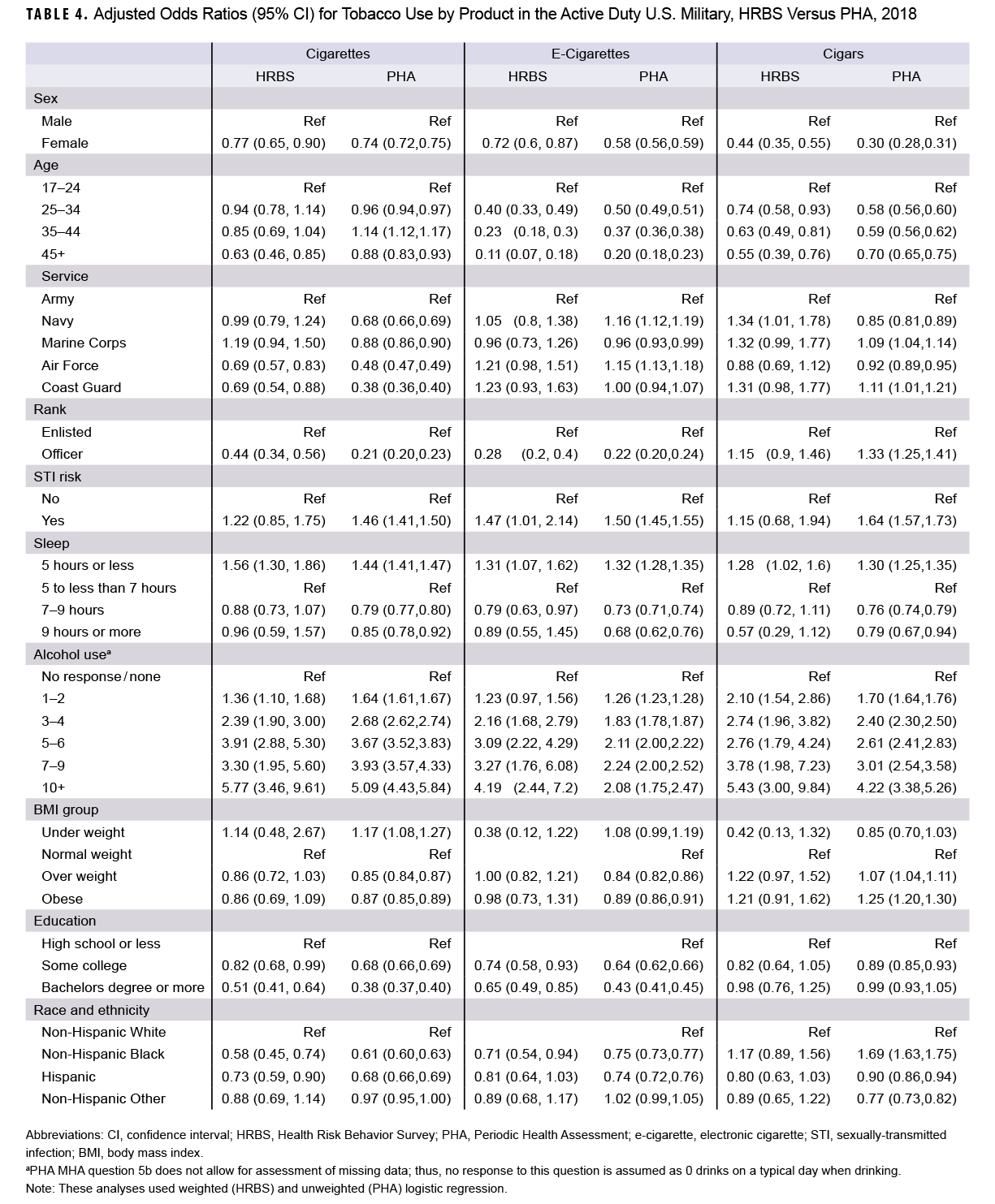
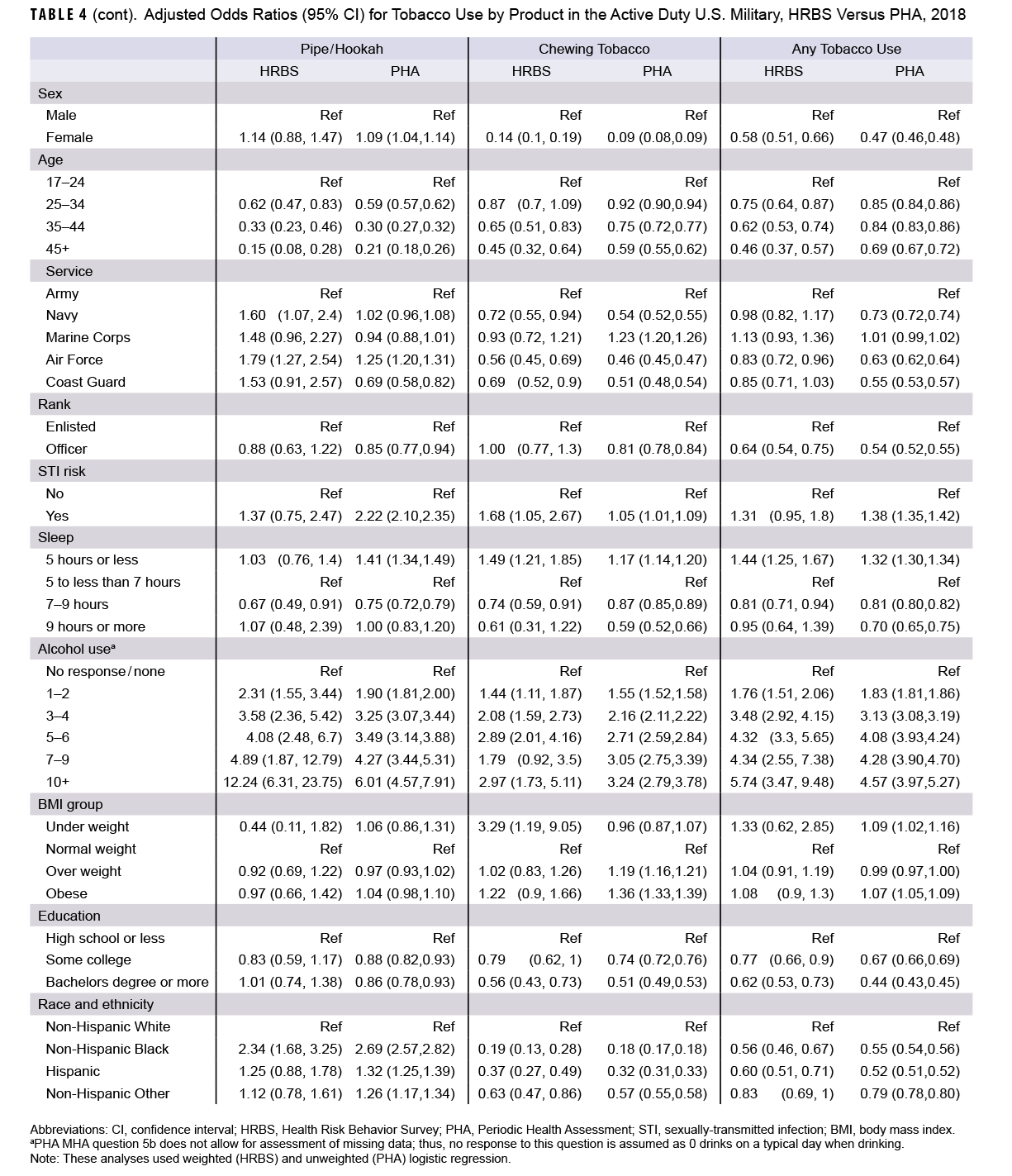
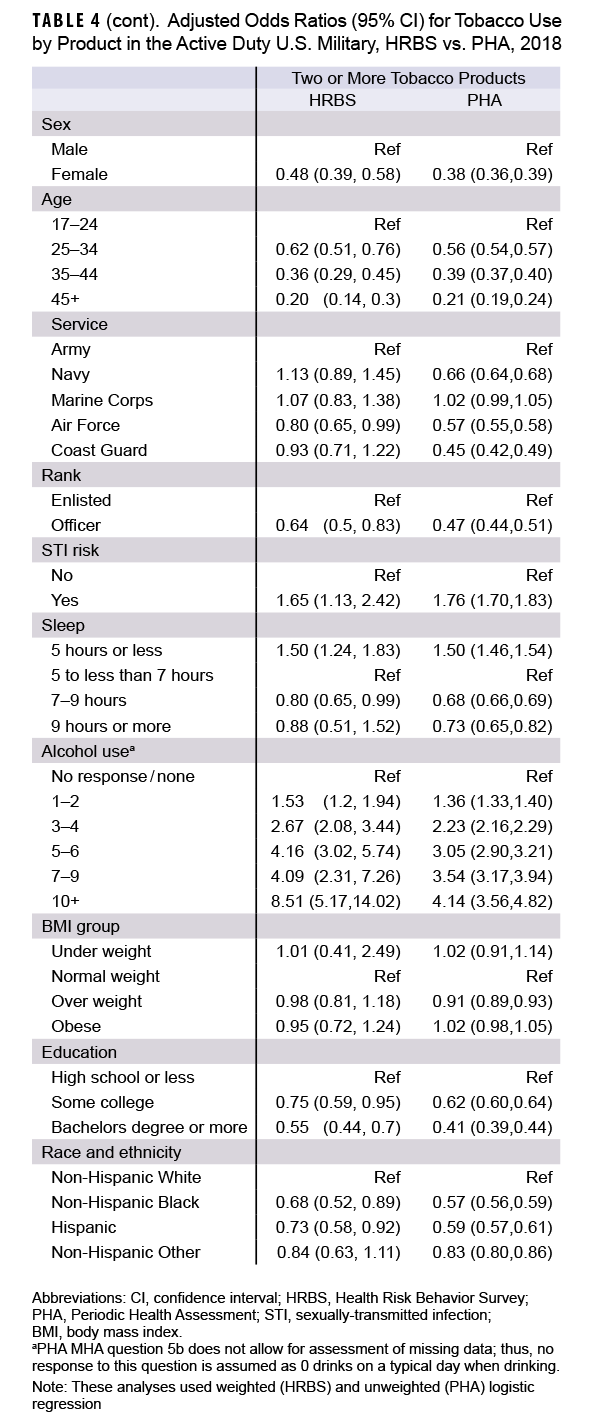
Table 4 shows the relationship between each demographic and behavioral factor and the different types of tobacco or nicotine use after adjusting for all other factors, which resulted in generally similar associations as seen in Table 3. HRBS data demonstrated statistically significant decreases in adjusted odds of any tobacco or nicotine use among service members who were female, older, officers, with higher education levels, had more hours of sleep per night, of a race or ethnicity other than Non-Hispanic White, and with lower alcohol use levels. The findings from PHA data were similar, but with even stronger negative associations between any use and female sex, service, officer rank, and increased education level. In contrast, negative associations of slightly lower magnitude were seen in the PHA data for increasing age, while positive associations of slightly lower magnitude were seen for alcohol use.
Discussion
Service members consistently reported much lower prevalence for all types, and combinations, of tobacco or nicotine use in the PHA compared to the HRBS. As reported elsewhere, HRBS data trends from 2015 to 2018 indicate increased prevalence of cigarette use (13.8% to 18.4%) and e-cigarette use (12.4% to 16.2%) in the U.S. military.5,1 Highest prevalence for both types of tobacco or nicotine use was among 17-24 year olds, whose cigarette use increased from 19.3% to 23.1%, and e-cigarette use rose from 22.8% to 27.9%.5 Factors demonstrating generally strong associations with most or all types of increased tobacco and nicotine use included younger age, male sex, enlisted rank, lower education level, greater amounts of alcohol use, increased STI risk, and Marine Corps service. While associations between tobacco or nicotine use and demographic and behavioral variables were mostly similar in the two surveys, there were some inconsistent associations with branch of service.
The HRBS-obtained prevalence of cigarette use in the U.S. military was lower in 2015 than the prevalence in the general U.S. population reported by the U.S. Centers for Disease Control and Prevention,5,9 but HRBS-obtained prevalence then increased in 2018 to exceed the U.S. population (18.4% vs. 13.7%, respectively).10 In contrast, the 2018 prevalence of cigarette use in the U.S. military estimated from PHA data (11.1%) was lower than U.S. population prevalence. As the methods employed in obtaining HRBS data were more similar to those used by the CDC for civilian data than in PHA data capture, HRBS data were preferentially utilized for the remainder of military and civilian comparisons. The prevalence of e-cigarette use also remained much higher in the U.S. military than in the U.S. population (16.2% compared to 3.2%),10 as in 2015.5 “Any smoking” was higher among service members than in the U.S. population (37.8% vs. 19.7%), as was use of two or more tobacco or nicotine products (17.4% vs. 3.7%).9
Among 17-24 year olds in the U.S. military there was a much higher prevalence (23.1%) of cigarette use found than in the U.S. 18-24 year old population (7.8%).10 The U.S. military also had a much higher prevalence of e-cigarette use in the 17-24 age group (27.9% vs. 7.6% in the U.S. population). Any smoking was higher among 17-24 year old service members than in the U.S. population (45.7% vs. 17.1%), as was use of two or more tobacco or nicotine products (25.7% vs. 4.1%). The prevalence of e-cigarette use among U.S. high school students (20.8%) in 2018 was closer to the prevalence among the youngest U.S. service members (27.9%), compared to the U.S. population of the same age (7.6%), but U.S. high school student cigarette use (8.1%) was much lower than cigarette use by youngest U.S. service members (18.4%).11
The findings in this study are generally similar to the findings of the 2015 HRBS, but the differences between the military and civilian populations are of greater magnitude.5 The 7.3% prevalence estimate of e-cigarette use among ACSMs from the PHA data in this study was similar to the 9% prevalence among active and reserve service members previously reported, also using 2018-2019 PHA data.12 Similar to this study, in 2018 the prevalence of e-cigarette use among U.S. Air Force recruits increased to 15.3%, although prevalence of cigarette and other tobacco or nicotine product use decreased in that study but increased in this study.13 This study also found similar factors associated with higher prevalence of tobacco or nicotine use, as reported in previous military studies, including younger age, male sex, enlisted rank, lower education levels, greater alcohol use, and Army or Marine Corps service.5,14 Similar associations have also been found among the general U.S. population.10
The most important strengths of this study are the large sample sizes, multiple data sources to assess the burden of tobacco and nicotine use in the U.S. military, and the comparability between the two sources due to similar survey questions. The stratified random survey design of the HRBS is also a contributing strength, as it provides estimates representative of the entire U.S. military population.
This work also has several important limitations. Tobacco and nicotine use have been highly dynamic in both the U.S. general and military populations in recent years, and trends have likely changed since 2018; the release of the 2024 HRBS should allow further assessment of these trends. The weighted response rate for the 2018 HRBS was low (9.6%), which could introduce selection bias into these estimates if participating service members differed from those not participating1; this type of volunteer bias in survey literature generally leads to healthier participants, however, so tobacco and nicotine use estimates obtained through HRBS data utilization would have been expected to underestimate prevalence, not overestimate it.15 Likewise, the 64% of service members for whom PHA data were available may have differed from those for whom data were unavailable, but because how those service members differed is unknown, the impact of this difference on prevalence estimates is unknown.
A more important source of PHA underestimation is introduction of misclassification bias if participants did not provide accurate information on their tobacco and nicotine use, which could occur due to social desirability bias, perceived stigma of tobacco and nicotine use, or other perceived negative consequences of divulging tobacco and nicotine use behaviors to other military personnel during a required military exam documented on an official form.16 The much lower prevalence for all types of tobacco and nicotine use in PHA data compared to the HRBS suggests this misclassification may lead to substantial bias and underestimates of the burden of tobacco and nicotine use.
Some misclassification may be non-differential; for example, the smaller aORs for age and alcohol use using PHA data compared to HRBS data suggest bias towards the null and possible non-differential misclassification. The more extreme aORs in the PHA data for other variables such as Naval service, sex, rank, and education compared to HRBS data do suggest possible differential misclassification, which could occur if service members who were female, officers, higher educated, and serving in the Navy were more affected by social desirability, stigma, or perceived negative consequences due to reporting tobacco and nicotine use.4 The assessment of other health behaviors such as alcohol use, drug use, and sexual practices may also be biased (particularly in the PHA) due to perceived stigma and potential for negative career consequences.17 The magnitude of this misclassification bias may be associated with the amount of stigma and potential consequences perceived for each behavior, so further research should consider and study their possible associations.
Tobacco and nicotine use remain an important threat to the health of U.S. military service members, resulting not only in short- and long-term health consequences, but also billions of dollars in health care and lost productivity costs,8 decreased fitness,18 and higher rates of premature discharge.19 Military tobacco and nicotine control policies and interventions must be guided by accurate and timely surveillance to ensure interventions are effective and responsive to dynamic societal, cultural, and economic forces that affect tobacco and nicotine use.
This study suggests that the PHA can provide timely information on trends in military tobacco and nicotine use over time, but much higher estimates in this study obtained from the confidential, voluntary HRBS also suggest that the command-directed PHA, which is part of a service member’s permanent record, may substantially underestimate the prevalence of all types of tobacco and nicotine use. Additionally, the more extreme differences between some types of service members suggest that this misclassification may be differential. This issue could potentially result in biased, and thereby invalid, associations with these demographic and behavioral risk factors, such as service members who are female, officers, higher educated, or serve in the Navy.
These differences also suggest that HRBS tobacco and nicotine use questions should not be discontinued, as some have suggested,1 since its data may be more valid than the PHA. The HRBS, on the other hand, suffers from a lack of timeliness, as it is only performed every three to six years, with its data lagging several years. Both data sources provide uniquely valuable information to guide military force health protection and readiness policy, and they should be used in tandem. Further research is needed to assess the validity of PHA data, not only for tobacco and nicotine use but other important health behaviors and outcomes as well.
Disclaimers
The contents of this publication are the sole responsibility of the authors and do not necessarily reflect the views, assertions, opinions, nor policies of the Uniformed Services University of the Health Sciences, the Defense Health Agency, or the Department of Defense.
Acknowledgments
The authors would like to thank Ms. Jessica H. Murray, MPH for the PHA data analysis presented in this report.
References
- Meadows SO, Engel CC, Collins RL, et al. 2018 Department of Defense Health Related Behaviors Survey (HRBS); Results for the Active Component. RAND Corporation; 2021. Accessed Aug. 28, 2022. https://www.rand.org/pubs/research_reports/RR4222.html
- Office of the Under Secretary of Defense for Personnel and Readiness. DOD Instruction 6025.19: Individual Medical Readiness Program. Department of Defense. Updated Jul. 13, 2022. Accessed Dec. 24, 2023. https://www.esd.whs.mil/portals/54/documents/dd/issuances/dodi/602519p.pdf
- Office of the Under Secretary of Defense for Personnel and Readiness. DOD Instruction 6200.06: Periodic Health Assessment (PHA) Program. Department of Defense. Updated Sept. 8, 2016. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/620006p.pdf
- Nelson JP, Pederson LL, Lewis J. Tobacco use in the Army: illuminating patterns, practices, and options for treatment. Mil Med. 2009;174(2):162-169. doi:10.7205/milmed-d-01-2008
- Keltner CH, Kao TC, Ahmed A, Mancuso JD. E-cigarette and dual product use as an emerging health threat to the US military. Tob Prev Cessat. 2021;7:43. doi:10.18332/tpc/135516
- Grier T, Knapik JJ, Canada S, Canham-Chervak M, Jones BH. Tobacco use prevalence and factors associated with tobacco use in new U.S. Army personnel. J Addict Dis. Jul 2010;29(3):284-293. doi:10.1080/10550887.2010.489445
- Smith B, Ryan MA, Wingard DL, et al. Cigarette smoking and military deployment: a prospective evaluation. Am J Prev Med. 2008;35(6):539-546. doi:10.1016/j.amepre.2008.07.009
- Institute of Medicine of the National Academies. Combating Tobacco Use in Military and Veteran Populations. The National Academies Press; 2009. http://www.nap.edu/catalog/12632/combating-tobacco-use-in-military-and-veteran-populations
- Phillips E, Wang TW, Husten CG, et al. Tobacco product use among adults–United States, 2015. MMWR Morb Mortal Wkly Rep. 2017;66(44):1209-1215. doi:10.15585/mmwr.mm6644a2
- Creamer MR, Wang TW, Babb S, et al. Tobacco product use and cessation indicators among adults–United States, 2018. MMWR Morb Mortal Wkly Rep. 2019;68(45):1013-1019. doi:10.15585/mmwr.mm6845a2
- Gentzke AS, Creamer M, Cullen KA, et al. Vital signs: tobacco product use among middle and high school students–United States, 2011-2018. MMWR Morb Mortal Wkly Rep. 2019;68(6):157-164. doi:10.15585/mmwr.mm6806e1
- Gill AA, Alford B, Balmer J, et al. Use of electronic cigarettes among U.S. military service members–prevalence and associated risk factors. Subst Abus. 2022;43(1):1300-1307. doi:10.1080/088970 77.2022.2095075
- Little MA, Fahey MC, Wang XQ, et al. Trends in tobacco use among young adults presenting for military service in the United States Air Force between 2013 and 2018. Subst Use Misuse. 2021;56(3):370-376. doi:10.1080/10826084.2020.1868517
- Lin J, Zhu K, Hoang PK, et al. Electronic cigarette use and related factors among active duty service members in the U.S. military. Mil Med. 2020;185(3-4):418-427. doi:10.1093/milmed/usz267
- Andreeva VA, Salanave B, Castetbon K, et al. Comparison of the sociodemographic characteristics of the large NutriNet-Sante e-cohort with French census data: the issue of volunteer bias revisited. J Epidemiol Community Health. 2015;69(9):893-898. doi:10.1136/jech-2014-205263
- Cantrell J, Hair EC, Smith A, et al. Recruiting and retaining youth and young adults: challenges and opportunities in survey research for tobacco control. Tob Control. 2018;27(2):147-154. doi:10.1136/tobaccocontrol-2016-053504
- Beltran RM, Schuyler AC, Blair CS, et al. “That’s kind of like the big struggle right now is can we get PrEP?”: facilitators and barriers to PrEP uptake among active duty gay and bisexual men. Sex Res Social Policy. 2023;20(2):413-425. doi:10.1007/s13178-021-00622-6
- Feinberg JH, Ryan MA, Johns M, et al. Smoking cessation and improvement in physical performance among young men. Mil Med. 2015;180(3):343-349. doi:10.7205/MILMED-D-14-00370
- Klesges RC, Haddock CK, Chang CF, Talcott GW, Lando HA. The association of smoking and the cost of military training. Tob Control. 2001;10(1):43-47. doi:10.1136/tc.10.1.43