Early awareness of cases of infectious disease facilitates timely implementation of control measures and policies to prevent disease or reduce spread. To support force health protection, the Electronic Surveillance System for the Early Notification of Community-based Epidemics (ESSENCE)1 collects near real-time biosurveillance data globally on U.S. military personnel. ESSENCE systematically queries millions of health encounters to detect records of potential public health importance. Statistical algorithms detect unusual increases, alerting public health staff to findings that may warrant investigation.1 ESSENCE receives several types of data including outpatient health encounter records from U.S. Military Health System (MHS) facilities, pharmacy prescriptions, laboratory results, and radiology reports. This report describes how ESSENCE contributed to case detection from the onset of the mpox outbreak.
The U.S. government declared mpox a national public health emergency on August 4, 2022.2 Nearly 3 months earlier, on May 13, 2022, the World Health Organization (WHO) was notified of a cluster of 3 mpox cases from a single household in the United Kingdom. These cases were suspected to be locally acquired; 2 days later 4 additional cases were reported by sexual health clinics, all among male patients who have sex with men.3 By May 21, 2022, locally acquired cases of this zoonotic disease had been confirmed in 11 other non-endemic countries including the U.S.4
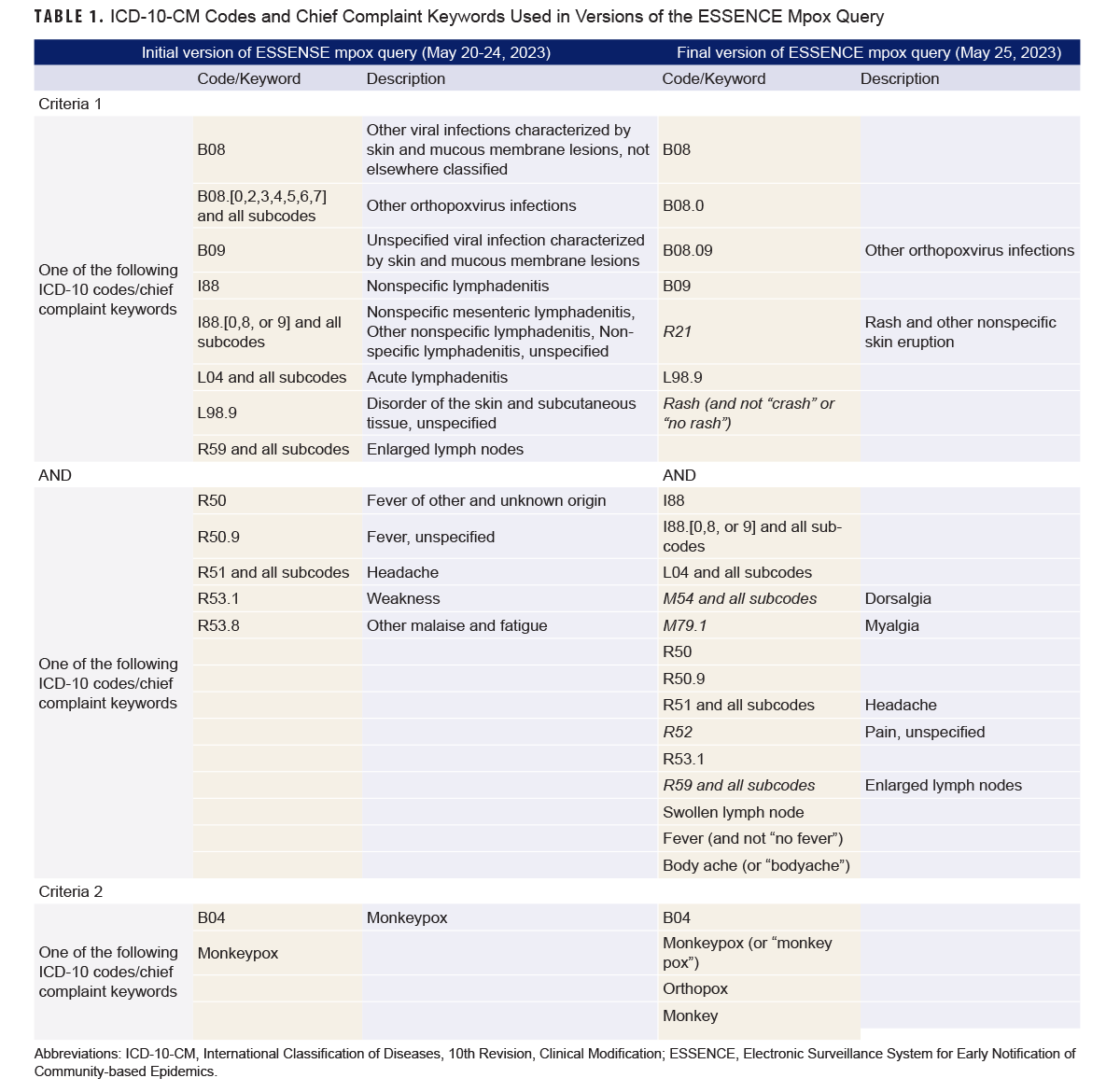
To detect specific health events, queries in ESSENCE are typically constructed with chief complaint keywords or codes from the International Classification of Diseases 10th Revision, Clinical Modification (ICD-10-CM) linked by logical operators (e.g., “and”, “or”). An initial mpox query was developed on May 20, based on known symptoms and specific criteria for discharge diagnosis ICD-10-CM codes and chief complaint keywords (Table 1).
While ESSENCE is designed to support surveillance and outbreak detection, the system’s performance should be evaluated when utilized during a public health response. This report describes how ESSENCE was used to monitor the mpox outbreak, assesses the system’s performance to detect confirmed/probable cases among MHS beneficiaries during May–August 2022, and describes approaches for improving system performance and utilization.
Methods
The initial mpox ESSENCE query was modified 5 days after its creation, to align with the WHO case definition for suspected cases (lowest threshold to meet the case criteria), followed by a minor change to additionally capture the keyword “monkey” without “pox” due to frequent misspellings (Table 1).5 Potential mpox cases included all health encounters that met the query criteria. Encounters with a discharge diagnosis ICD-10-CM code for diaper rash or hand, foot, and mouth disease, a chief complaint mentioning monkey bars, or a missing Electronic Data Interchange Personal Identifier (EDI-PI) were excluded as potential cases.
To assess the performance of the final version of the ESSENCE mpox query results, potential cases identified from May 1 through August 31, 2022 were compared to a validated master case list maintained by the Armed Forces Health Surveillance Division (AFHSD) Integrated Biosurveillance (IB) Branch. Epidemiologists at AFHSD IB created the master case list by compiling information about potential cases from various sources including the ESSENCE mpox query, reportable medical events (RMEs) from the Disease Reporting System internet (DRSi),6 service-specific reporting to AFHSD, notifications from stakeholders who received weekly case count reports, as well as direct informal communications. AFHSD IB epidemiologists contacted the appropriate Defense Center for Public Health (DCPH) to inform them of potential cases and request additional information. To validate the master case list, AFHSD IB epidemiologists reviewed electronic medical records of potential cases using Armed Forces Health Longitudinal Technology Application (AHLTA) to gather epidemiological, laboratory, and clinical information. CDC case definitions were used to classify potential cases as confirmed, probable, suspect, or not a case.7 Starting in July, the master case list was cross-checked daily with Defense Health Agency (DHA) Composite Health Care System and MHS GENESIS medical records in which mpox was recorded as a diagnosis, using reports provided by DHA administrative personnel. Results from 2 simpler, alternative queries, B04 ICD-10-CM code (alternative query 1 [AQ1]) and B04 ICD-10-CM code (AQ2) or mention of “monkey” in the chief complaint, were also compared with the mpox master case list to evaluate potential approaches to improve case detection. These queries were not implemented during the mpox outbreak but were retrospectively reviewed.
Results
A total of 3,067 unique encounters, from 2,750 unique individuals, as determined by EDI-PIs, were detected between May 1 and August 31, 2022. ESSENCE mpox surveillance of MHS beneficiaries was initiated earlier, on May 1, than U.S. mpox case reporting, on May 17 (Figure 1).
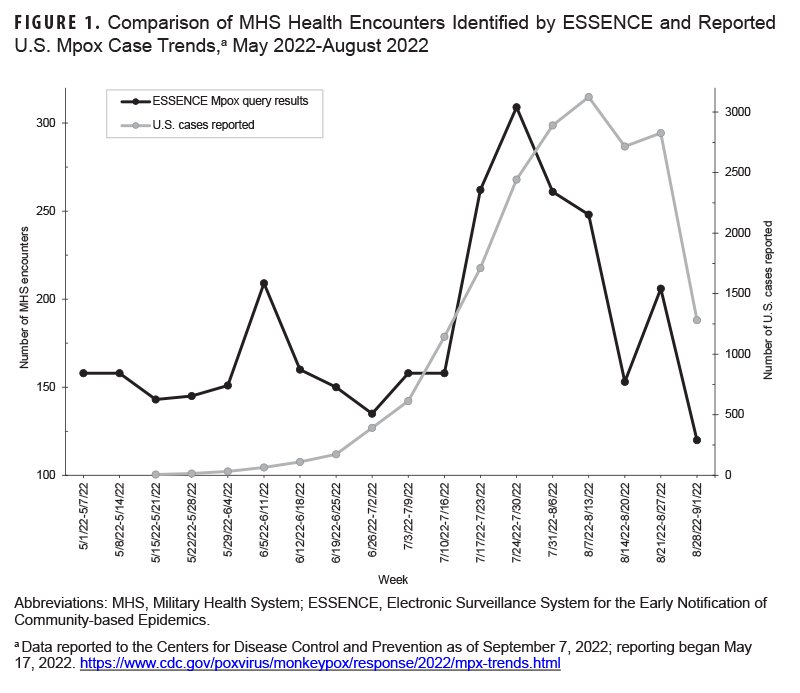
The peak in the total number of health encounters returned by the mpox query preceded the peak in reported U.S. cases by 2 weeks. The first confirmed case of mpox among MHS beneficiaries was detected as a potential case by the ESSENCE mpox query 5 days prior to laboratory confirmation (Figure 2).
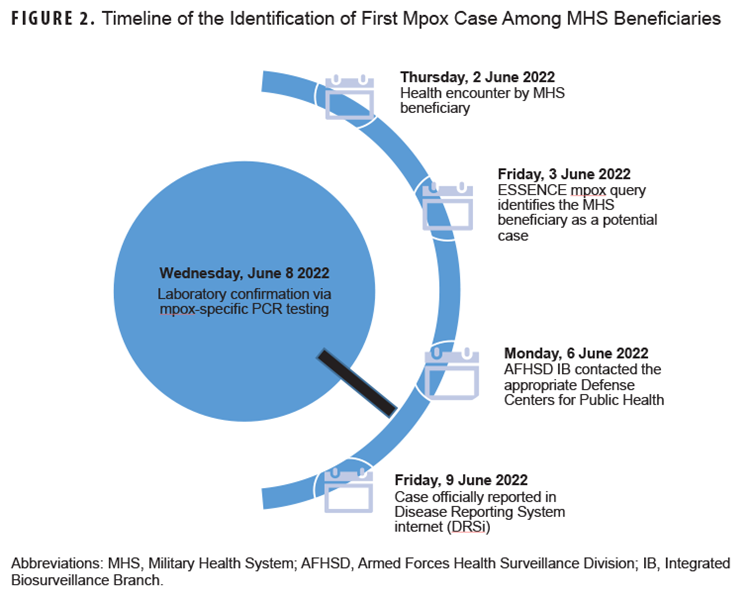
The patient, an active duty service member in Germany, developed symptoms in late May, and reported no travel within the previous 90 days.
Table 2 summarizes the ESSENCE mpox query results by validated, master list case status and compares its results to those from the alternative queries (AQs).
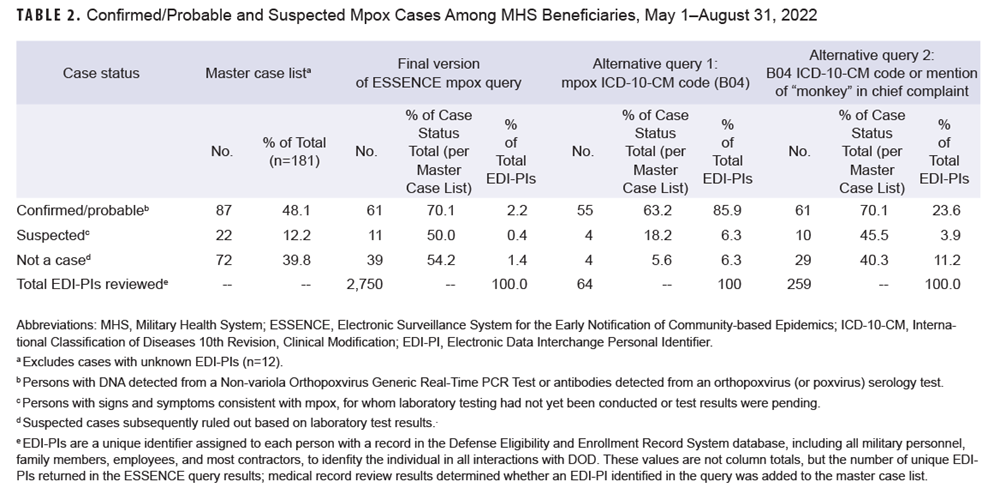
The ESSENCE mpox query detected 70.1% of confirmed/probable mpox cases based on a review of medical records for 2,750 individuals. AQ1 and AQ2 reduced the number of potential cases requiring medical record review (64 and 259, respectively), while still detecting 63.2% and 70.1% of confirmed/probable cases, respectively. The positive predictive value (PPV) of the ESSENCE mpox query was 2.2% (61/2,750). AQ2 had a higher PPV, at 23.5% (61/259), with equal sensitivity. AQ1 had the highest PPV, 85.9% (55/64), but was less sensitive, detecting 6 fewer confirmed/probable cases.
Discussion
The time series plot of ESSENCE mpox query encounter counts closely tracked the U.S. outbreak peak late in the summer of 2022. The CDC’s U.S. data included MHS beneficiary case data, as mpox is a nationally notifiable condition as well as a DOD RME. ESSENCE detected the first confirmed mpox case among MHS beneficiaries 5 days prior to laboratory confirmation and 6 days prior to reporting in DRSi. Detection was facilitated by the inclusion of the ICD-10-CM code for mpox (B04) in the discharge diagnosis prior to laboratory confirmation. Practitioners may use this code broadly to indicate a clinically suspected or confirmed case, exposure, or testing.
The development and usefulness of queries to detect health events of interest is challenging when associated signs or symptoms are nonspecific or shared with other health events (i.e., many potential ICD-10-CM codes), or the code(s) do not yet exist (e.g., novel diseases, unknown etiology), or are not unique. Many potential cases detected by the mpox query were ultimately ruled out based on medical record review, or subsequent test results or alternate diagnoses (i.e., not a case) despite initial clinical suspicion. Depending upon the health event, the latter group may still be useful for public health detection.
Reviewing the medical records for 2,750 potential cases detected by the mpox query was time-intensive (5-10 minutes per record) and completing a review the same day as detection became unfeasible for a single, dedicated reviewer. The cost, in both time and effort, could make the approach impractical in many outbreak scenarios or not worth the benefit, given that opting for AQ2 would have reduced the number of records for review by more than 10-fold, without sacrificing identification of true positive cases.
ESSENCE queries can easily be modified as knowledge of the disease epidemiology evolves, transmission patterns change, and case definitions are updated. Adjustments to the query, to reduce potential cases requiring review, must be carefully evaluated, as it could lead to confirmed cases being missed, as the AQ1 results demonstrate. Over the course of the outbreak the number of encounters with chief complaints mentioning “monkeypox” increased as patients requested educational information or were offered or received the vaccine, especially when it became more widely available. The ESSENCE mpox query was subsequently modified by removing symptom keywords and including negation terms to exclude vaccination-related encounters and persons without exposure or symptoms seeking medical education. When the modified query was executed for the analysis period, it returned 430 unique encounters (246 unique EDI-PIs; PPV=20.2%) with a sensitivity of 100%.
The desired tolerance for the completeness of case capture should consider human resources, surveillance goals, and characteristics of the health event (e.g., incidence, disease epidemiology), among other factors. In contrast to the results of this study, a recent study of case definitions to identify COVID-19-related encounters among MHS beneficiaries found that inclusion of a greater number of ICD-10-CM codes increased sensitivity at the cost of specificity.8
The analyses in this report had several limitations. The mpox query likely underestimated the detection of potential cases and therefore missed detection of some confirmed/probable cases (i.e., decreased sensitivity) for several reasons. Data from MTFs using MHS GENESIS were initially received in ESSENCE following a lag of a month; beginning on July 28, 2022, data were received daily beginning with July 23 encounters, but were incomplete (approximately 10% of the expected number were received). The sensitivity of the mpox detection query is dependent upon the completeness and accuracy of the chief complaint and ICD-10-CM codes entered in the medical records. ESSENCE does not capture health encounters or testing for MHS beneficiaries at non-MHS facilities, which could mean that some confirmed/probable cases among MHS beneficiaries are missed (i.e., decreased sensitivity). The master case list likely underestimated the true number of confirmed/probable cases, as health encounter notes and test results for MHS beneficiaries visiting non-MHS facilities were often not available in AHLTA. The population most at risk of mpox infection, men who have sex with men, may be more likely to seek care outside MHS, which would lead to a true case rate higher than stated in the AFHSD master list. MHS GENESIS medical records were not reviewed, so some cases may have gone undetected and led to an underestimation of the true incidence. Once test results became available, some cases classified as suspected in this analysis may have subsequently been classified as confirmed/probable, or not a case, which may have led to underestimation of the sensitivities of confirmed/probable case detection queries.
During the mpox outbreak ESSENCE biosurveillance was centralized, with AFHSD IB conducting all aspects of query development, data review and extraction, and electronic medical record review for all MHS beneficiaries. More efficient biosurveillance utilizing ESSENCE would be decentralized, incorporating the 2 designated ESSENCE users required at each MTF9 to conduct ongoing data review and initiate public health investigations. These MTF ESSENCE users’ awareness of local events and collaboration with local public health and clinical staff for record reviews would expand resources for timely follow-up of potential cases. In a decentralized approach AFHSD IB would refine queries, receive and compile critical findings reported by local users or DCPH, and maintain and report the master case list results to key stakeholders. Valuable insights and refinements on the specific process could be informed by pilot programs between AFHSD and a DCPH or several MTFs. Advancing towards a decentralized MHS-wide approach would improve the effectiveness of the ESSENCE biosurveillance process, by employing the situational awareness of those closest to the location of a public health event, in collaboration with strategic oversight and technical support provided by AFHSD staff.
Author Affiliations
Armed Forces Health Surveillance Division, Integrated Biosurveillance, Silver Spring, MD (Dr. McGee, Dr. Russell, Ms. Metcalf-Kelly); Cherokee Nation Strategic Programs, Tulsa, OK (Dr. McGee).
References
- Burkom H, Loschen W, Wojcik R, et al. Electronic Surveillance System for the Early Notification of Community-Based Epidemics (ESSENCE): overview, components, and public health applications. JMIR Public Health Surveill. 2021;7(6):e26303. doi:10.2196/26303
- Biden-Harris Administration Bolsters Monkeypox Response; HHS Secretary Becerra Declares Public Health Emergency. August 4, 2022. Accessed August 17, 2022. https://www.hhs.gov/about/news/2022/08/04/biden-harris-administration-bolsters-monkeypox-response-hhs-secretary-becerra-declares-public-health-emergency.html
- World Health Organization. Monkeypox—United Kingdom of Great Britain and Northern Ireland. May 18, 2022. Accessed July 15, 2022. https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON383
- World Health Organization. Multi-country monkeypox outbreak in non-endemic countries. May 21, 2022. Accessed October 6, 2022. https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON385
- World Health Organization. Surveillance, case investigation and contact tracing for monkeypox: interim guidance, 22 May 2022. Accessed May 25, 2022. https://apps.who.int/iris/handle/10665/354486
- Armed Forces Health Surveillance Division. Armed Forces Reportable Events Guidelines and Case Definitions, 1 January 2020. Accessed October 4, 2022. https://www.health.mil/Military-Health-Topics/Health-Readiness/AFHSD/Reports-and-Publications
- Centers for Disease Control and Prevention. Case Definitions for Use in the 2022 Mpox Response. July 22, 2022. Accessed March 14, 2023. https://www.cdc.gov/poxvirus/mpox/clinicians/case-definition.html
- Evaluation of ICD-10-CM-based case definitions of ambulatory encounters for COVID-19 among Department of Defense health care beneficiaries. MSMR. 2022;29(5):12-16.
- Department of Defense (DOD). Instruction 6200.03 Public Health Emergency Management (PHEM) Within the DOD. March 28, 2019. Accessed March 14, 2023. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/620003p.pdf