By Holly N. O'Reilly, Ph.D.
Nov. 9, 2020
 PHCoE graphic
PHCoE graphic
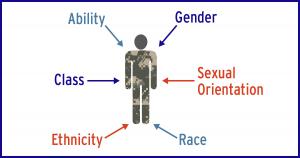
The term intersectionality, coined by Kimberle Williams Crenshaw, is used to describe how race, class, gender, and other individual characteristics intersect and overlap with one another. Intersectionality considers the ways that identities related to multiple socially constructed categories create unique sets of experiences, which are qualitatively different than the sum of individual categories of identity (American Psychological Association Dictionary). The idea of intersectionality is not new but is important to revisit within the context of the American military due to the demographic diversity among service members, many of whom have more than one identity characteristic (e.g., female, ethnic minority, disabled person or member of the LGBT community).
Awareness of intersectionality may help provide clinicians a lens through which to improve our understanding of each patient's unique story and the potential impact on patients who experience a more marginalized sense of identity. Social constructs (i.e., gender, race, and ethnicity) impact individuals psychologically. Having multiple identities leads to an idiosyncratic experience and may lead to unique types of oppression. By understanding and acknowledging the impact of co-occurring characteristics of identity, clinicians can improve our understanding of patients' experiences and contribute to improved therapeutic alliances.
Microaggressions
One way to understand the daily impact of intersectionality is through microaggressions. Microaggressions are defined as the everyday, subtle, intentional — and oftentimes unintentional — interactions or behaviors that communicate some sort of bias toward historically marginalized groups. Gender, racial and sexual orientation microaggressions are brief, everyday exchanges that send denigrating messages to people because they belong to a minority group or group of marginalized people. These statements and acts serve to diminish and dehumanize and may contribute to self-silencing of feelings of anger and resentment.
Because microaggressions may or may not be intentional, there are a number of challenges to address if a patients discloses experiencing microaggressions in treatment. It may help to identify and acknowledge the subtlety of the offense. Clinicians may encourage patients to share their dilemma surrounding the decision whether or not to confront the offending party and the potential consequences of doing so. Clinicians should also acknowledge the resulting emotional injury particularly when a patient feels that the microaggression may have a lasting impact on their aspirations or goals.
It's important to note that anyone can perpetrate or experience a microaggression. Research suggests that microaggressions are commonly experienced by patients in psychotherapy. For example, clinicians making statements of color blindness (e.g., "I don't see color") may serve to minimize the experience of people of color and may be seen as denying their experience of oppression. Making assumptions about a behavior or characteristic can also be a microaggression. Remember that it is better to ask the question rather than assume.
What can I do to incorporate intersectionality in practice?
Start by asking your patient additional assessment questions to get a better sense of their lived experience.
- Consider asking your patient how you can help. This will help you to explore their expectations of treatment and your role in therapy.
- Consider asking them to share their thoughts about the origins of the presenting problem. This line of questioning may tap into cultural issues or spiritual beliefs that may help explain their experience of the issue.
- Consider asking them directly about their lived experience. For example, "What is it like to be the first black female in your unit? Can you tell me more about your experience as the only gay person on your team?"
- If you inadvertently make an offensive statement in therapy, acknowledge the error, apologize, and make an effort to not repeat the mistake. As with other therapeutic alliance ruptures, authenticity can go a long way towards repairing the strain.
Resources
It is important to remember that we are all working on improving our cross-cultural competency skills and we all have room to improve. Start where you are and take time to learn more and expand your competence. You may consider these resources as you work to increase your cultural sensitivity and expand your skill set.
- National Institute of Mental Health fact sheets (also available in Spanish)
- Substance Abuse and Mental Health Services Administration training resources for work with the LGBT community
- Substance Abuse and Mental Health Services Administration Improving Cultural Competence guide
- Intersectionality and Cultural Competence presentation at last month's VA/DOD Women's Mental Health Webinar Series
Dr. O'Reilly is a clinical psychologist and sexual assault/sexual harassment SME at the Psychological Health Center of Excellence. She specializes in the consequences of psychological trauma and women's mental health.