Abstract
Malaria infection remains a potential health threat to U.S. service members located in or near endemic areas due to duty assignments, participation in contingency operations, or personal travel. This report summarizes findings from surveillance of malaria infections among U.S. service members in 2025 and analyzes trends for a 10-year period, from 2016 through 2025. In 2025, 36 cases of malaria were diagnosed among U.S. service members, representing a 12.5% increase from 32 cases reported in 2024. The majority of malaria cases occurred in service members who were male (94.4%), in the active component (80.6%), and serving in the Army (63.9%). Africa was the leading region of acquisition (n=14), primarily for P. falciparum infections. A significant 2025 finding is a shift in the predominant species to P. vivax, which accounted for 41.7% (n=15) of all cases, a notable increase from 10% of all cases in 2024. Most P. vivax cases (80.0%) were acquired in Korea. Seasonality of infection remained consistent, with 72.1% of cases diagnosed May through October. These findings underscore the critical need for continuous surveillance, strict command emphasis on personal protective measures, and region-specific prevention strategies to protect the health of the force and maintain military readiness.
What are the new findings?
Findings from 2025 indicate a 12.5% increase in malaria cases among U.S. service members compared to 2024, with a notable increase of new P. vivax cases. This change was driven almost entirely by P. vivax infections acquired in Korea, while Africa remained the principal source for P. falciparum cases.
What is the impact on readiness and force health protection?
The rise of P. vivax from Korea along with persistent P. falciparum infection from Africa not only directly affect force health protection but demonstrate a dynamic, regionally specific threat that requires specialized prevention strategies to maintain military readiness.
Background
Malaria has long posed a significant risk to U.S. military service members and operations.1 Before World War II, the disease was endemic across the southern U.S., prompting the 1942 establishment of the Office of Malaria Control in War Areas—an organization that would later become the Centers for Disease Control and Prevention—to mitigate vector-borne diseases around military installations.2 While this campaign was successful in the elimination of malaria as a public health threat to the U.S. by 1949, the disease remains a persistent risk to the operational readiness of U.S. service members when deployed to endemic tropical and subtropical regions.3-5
The risk to military personnel is heightened by operational realities, the emergence of drug-resistant parasites, and inconsistent adherence to preventive measures such as chemoprophylaxis and personal protective equipment.6-9 Travel to malaria-endemic regions, especially for foreign-born personnel visiting their countries of origin, also presents a significant medical concern.10-11 Studies have shown a significantly higher incidence of malaria in service members and their families with connections to malaria-endemic countries, particularly those from sub-Saharan Africa. This increased risk persists despite universal health coverage and access to pre-travel medical care for this specific population.11 Most human malaria cases are caused by 4 Plasmodium species—P. falciparum, P. vivax, P. malariae, and P. ovale—with P. falciparum and P. vivax the most significant. P. falciparum, found predominantly in Africa, is the most dangerous species, accounting for over 90% of malaria-related deaths,12 while P. vivax has the widest geographic distribution, with a high prevalence in Southeast Asia, the Western Pacific, and the Americas.13 These 2 species, P. falciparum and P. vivax, have distinct epidemiological profiles. A critical difference is the ability of P. vivax to cause relapses weeks or even months after initial infection,14 which occurs because the parasite can remain in the liver as hypnozoites, allowing dormant endemicity during the colder, mosquito-free seasons and extending its geographic range into temperate zones, such as the Korean peninsula.15
MSMR has published regular updates on malaria’s impact on service members since 1999. Current surveillance efforts include the differentiation of malaria types, such as the more lethal P. falciparum and relapsing P. vivax. This sustained surveillance provides critical data to inform force health protection strategy, and this update continues that mission by describing malaria’s epidemiological patterns among U.S. Armed Forces from 2016 through 2025.
Methods
The surveillance population for this report includes service members of the U.S. Army, Navy, Air Force, Marine Corps, Space Force, and Coast Guard. The surveillance period was January 1, 2016 through December 31, 2025. Records from the Defense Medical Surveillance System (DMSS) were searched to identify qualifying evidence of a malaria diagnosis from reportable medical events (RMEs), hospitalizations, outpatient encounters (in military and non-military facilities), and laboratory results from military facilities.
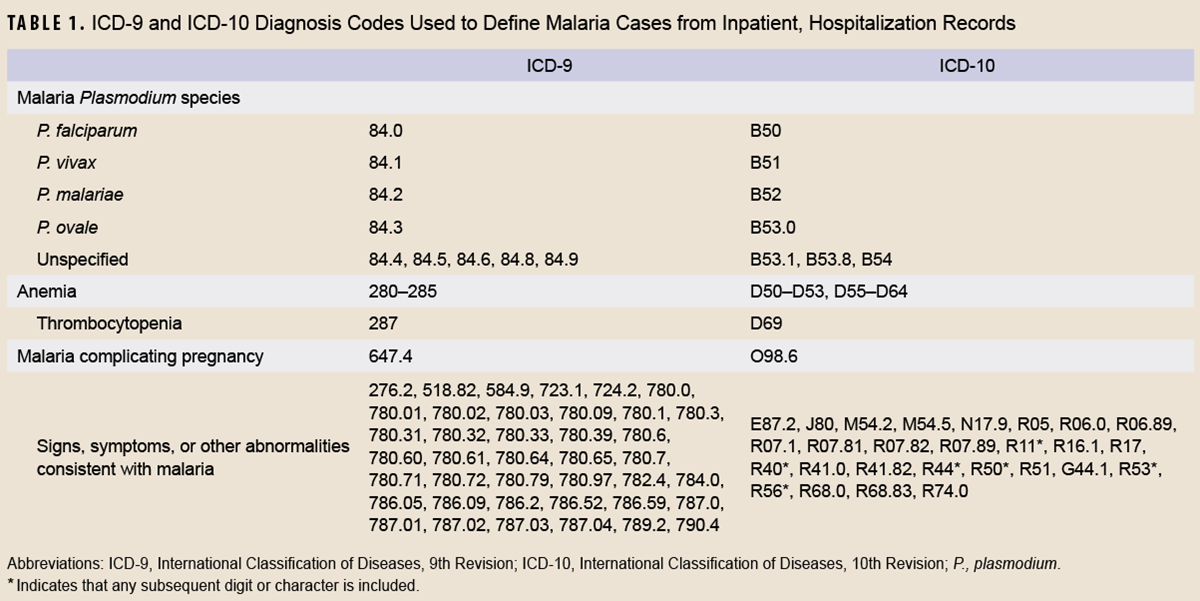
Case definition criteria for malaria included either 1) an RME record of confirmed malaria, 2) a hospitalization record with a primary diagnosis of malaria, 3) a hospitalization record with a non-primary diagnosis of malaria due to a specific Plasmodium species, 4) a hospitalization record with a non-primary diagnosis of malaria plus a diagnosis of anemia, thrombocytopenia, and related conditions, or malaria-complicating pregnancy in any diagnostic position, 5) a hospitalization record with a non-primary diagnosis of malaria plus diagnoses of signs or symptoms consistent with malaria in each diagnostic position preceding malaria, or 6) a positive malaria antigen test plus an outpatient record with a diagnosis of malaria in any diagnostic position within 30 days of the specimen collection date.16 The relevant International Classification of Diseases, 9th and 10th revisions (ICD-9/ICD-10) codes used to identify cases are shown in Table 1.
This analysis restricted each service member to 1 episode of malaria per 365-day period. When multiple records documented a single episode, the date of the earliest record was considered the date of clinical onset. Records within 30 days of the clinical onset date were reviewed for evidence of a Plasmodium species.
Presumed locations of malaria acquisition were estimated with a hierarchical algorithm: 1) cases diagnosed in a malaria-endemic country were considered acquired in that country, 2) RMEs that listed exposures to malaria-endemic locations were considered acquired in those locations, 3) RMEs not listing exposures to malaria-endemic locations but reported from installations in malaria-endemic locations were considered acquired in those locations, 4) cases diagnosed among service members during or within 30 days of deployment or assignment to a malaria-endemic country were considered acquired in that country, and 5) cases diagnosed among service members deployed or assigned to a malaria-endemic country within 2 years before diagnosis were considered acquired in those countries. All remaining cases were considered to have acquired malaria in unknown locations.
Results
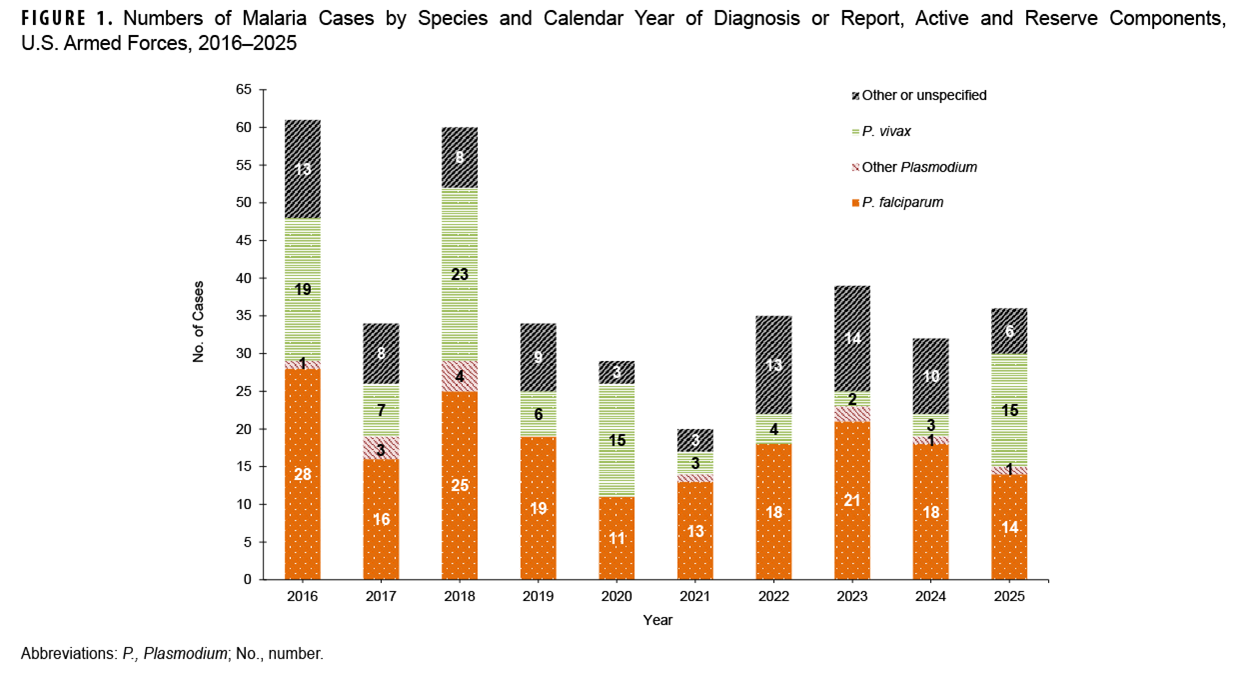
In 2025, a total of 36 U.S. service members were diagnosed with, or reported to have, malaria (Table 2). The annual total for 2025 represents a 12.5% increase in malaria cases from the 32 cases reported in 2024 (Figure 1). Twenty-eight (77.8%) of the 36 cases in 2025 were identified from RME records. The remaining 8 cases were identified through additional case definition criteria: 5 cases from hospitalization records with a defining diagnosis of malaria in the primary diagnostic position, 2 cases from hospitalization records with a case defining diagnosis of malaria in a non-primary diagnostic position due to a specific Plasmodium species or additional diagnoses for malaria-related conditions, and 1 case from a U.S. Department of War laboratory report of a positive malaria antigen test plus 1 outpatient medical encounter for a case-defining diagnosis of malaria in any diagnostic position within 30 days of the specimen collection date (data not shown).
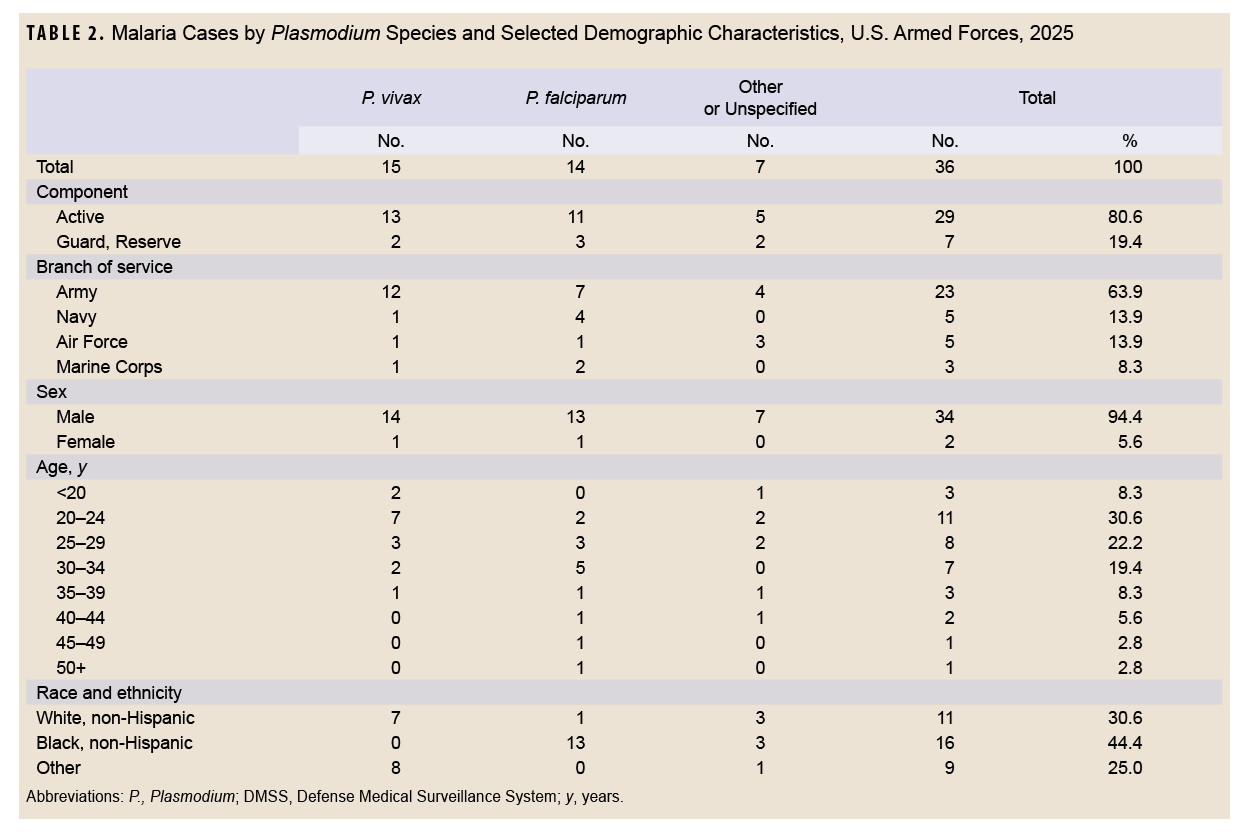
As in previous years, the majority of U.S. military members diagnosed with malaria in 2025 were men (94.4%), members of the active component (80.6%), and in the Army (63.9%). No cases were reported in the Space Force or Coast Guard. Non-Hispanic Black service members and individuals ages 20-24 years accounted for the most cases of malaria (44.4% and 30.6%, respectively) (Table 2).
Examination of the 28 malaria case records reported as RMEs in 2025 revealed that 5 of the case exposures were classified as deployment-related, 5 as duty-related (but not deployment-related), 10 were non-deployment and non-duty related, while 8 cases were missing exposure classification. Six of the 10 cases classified as non-deployment and non-duty related were documented as acquired in Africa (data not shown).
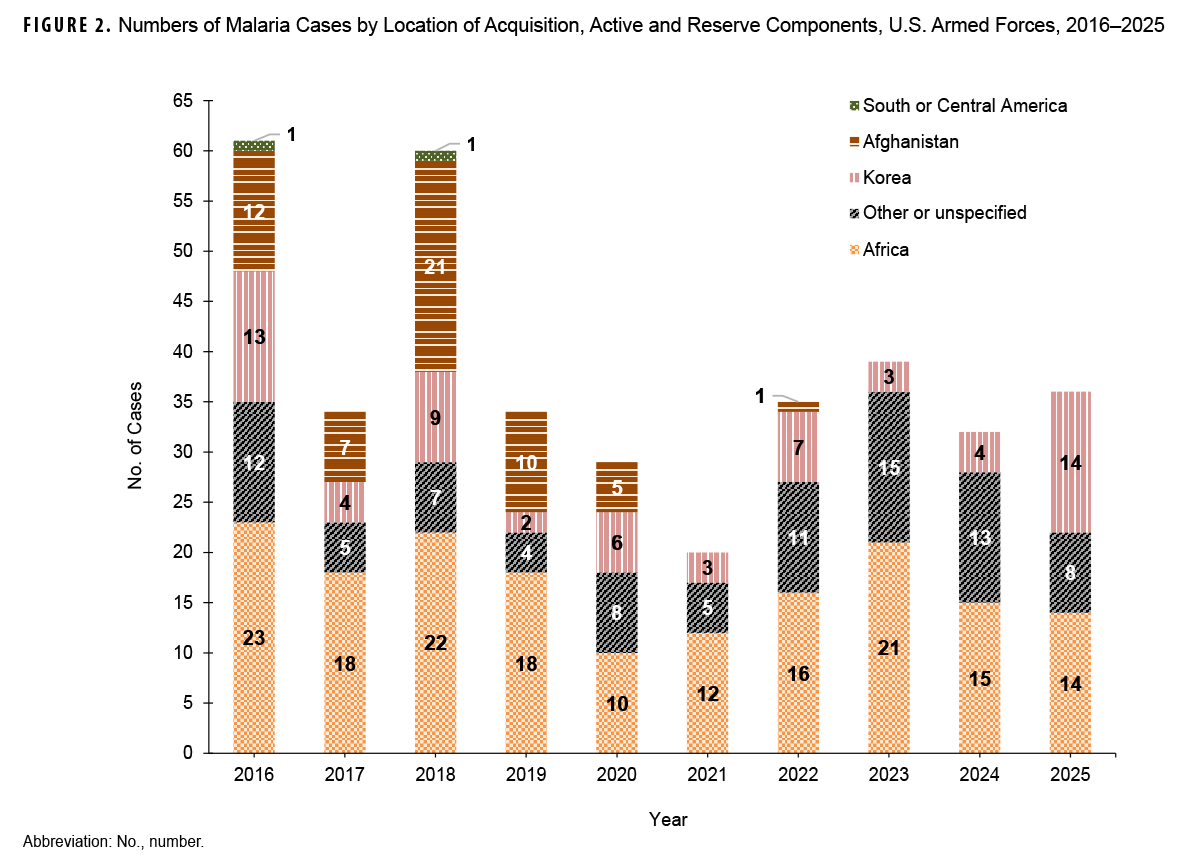
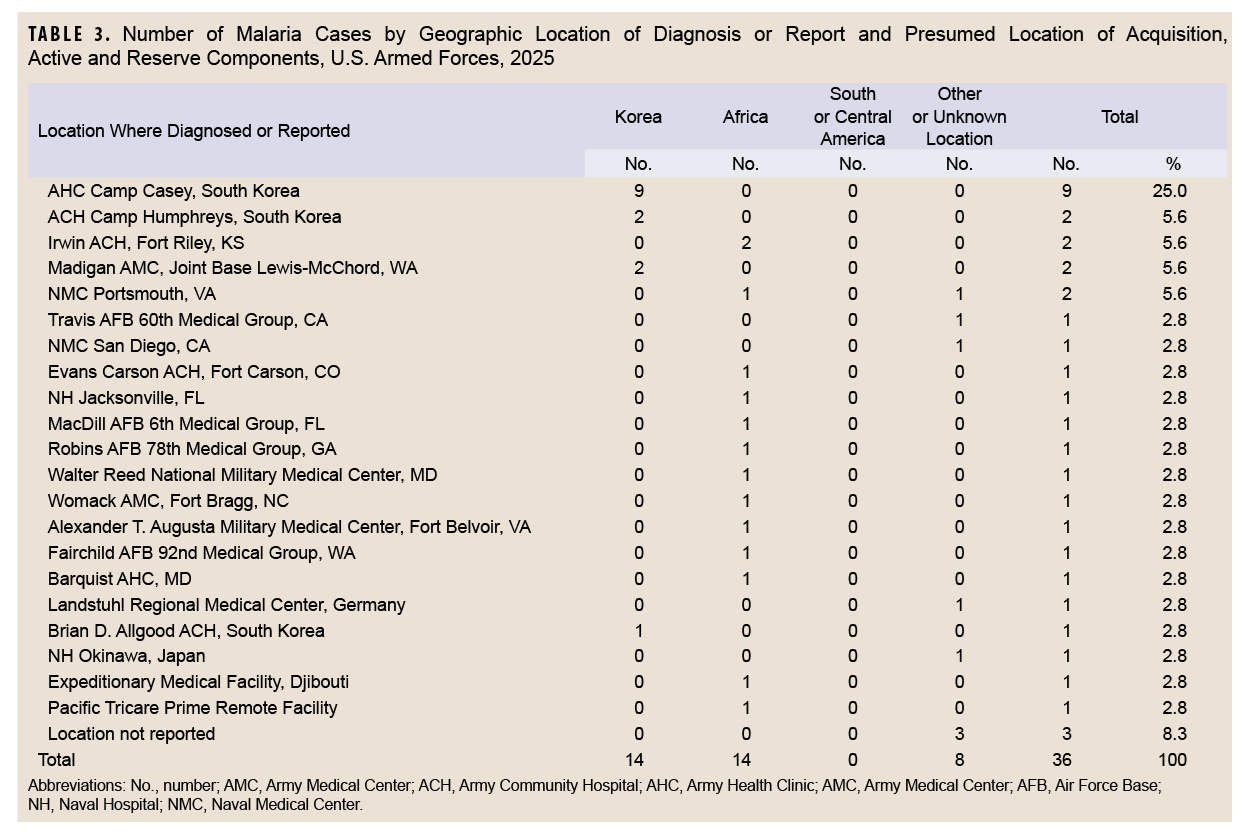
During the 2016-2025 surveillance period, malaria cases acquired in Africa (n=169, 44.5%) and other or unspecified locations (n=88, 23.2%) accounted for the largest numbers, followed by Korea (n=65, 17.1%), Afghanistan (n=56, 14.7%), and South and Central America (n=2, 0.5%) (Figure 2). Africa consistently reported the highest numbers of malaria cases throughout the period. Cases in Afghanistan peaked to 21 in 2018, thereafter declining to 0 cases during last 3 years of the surveillance period. Malaria cases were diagnosed or reported in 2025 from 21 different medical facilities: 14 facilities in the U.S., 3 facilities in the Republic of (South) Korea, and 1 facility each in Germany, Africa, and Japan, as well as 1 TRICARE Prime remote location (Table 3).
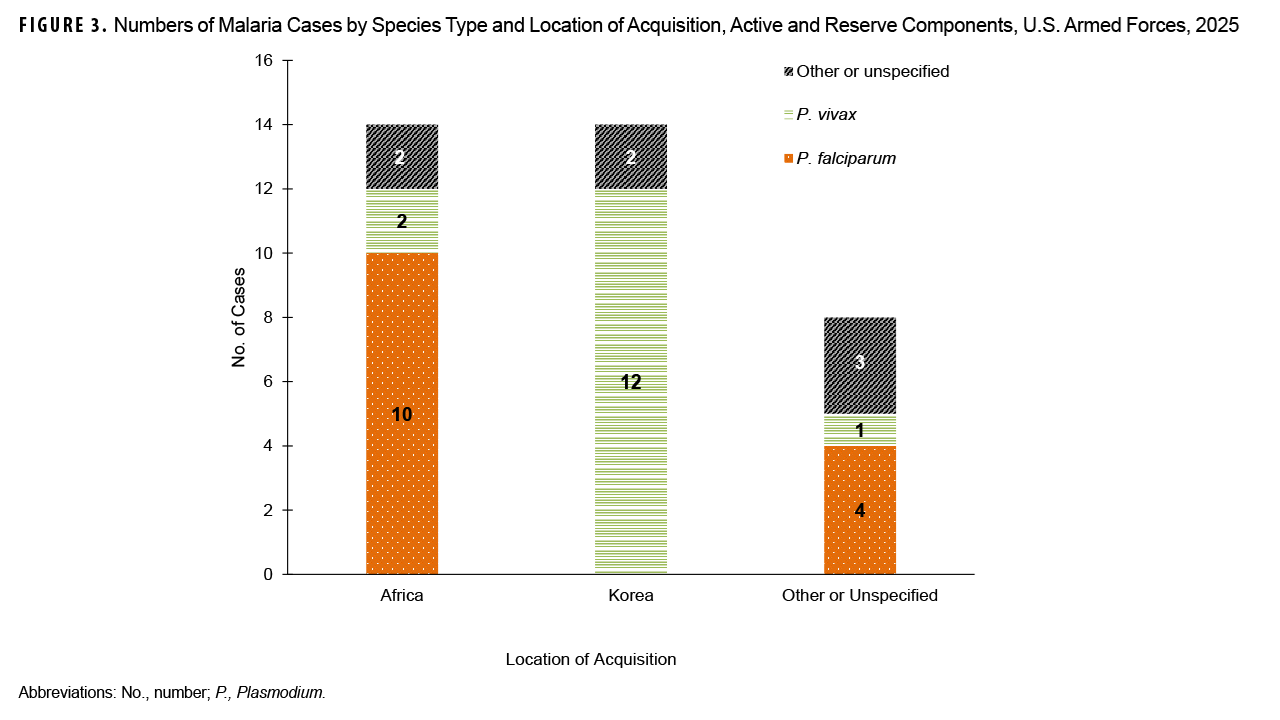
Most U.S. service member malaria cases in 2025 were caused by P. vivax (n=15, 41.7%). Twelve of those 15 P. vivax cases were acquired in Korea. The remaining cases were attributed to P. falciparum (n=14, 38.9%) and other or unspecified types of malaria (n=7, 19.4%). Most cases acquired in Africa (n=14) were caused by P. falciparum (n=10, 71.4%) (Figure 3). The 14 malaria cases acquired in Africa were associated with several countries, including Djibouti (n=3), Ghana (n=3), Cameroon (n=2), Nigeria (n=2), Sierra Leone (n=1), Guinea (n=1), and Tanzania (n=1); 1 case was associated with an unknown African location (data not shown).
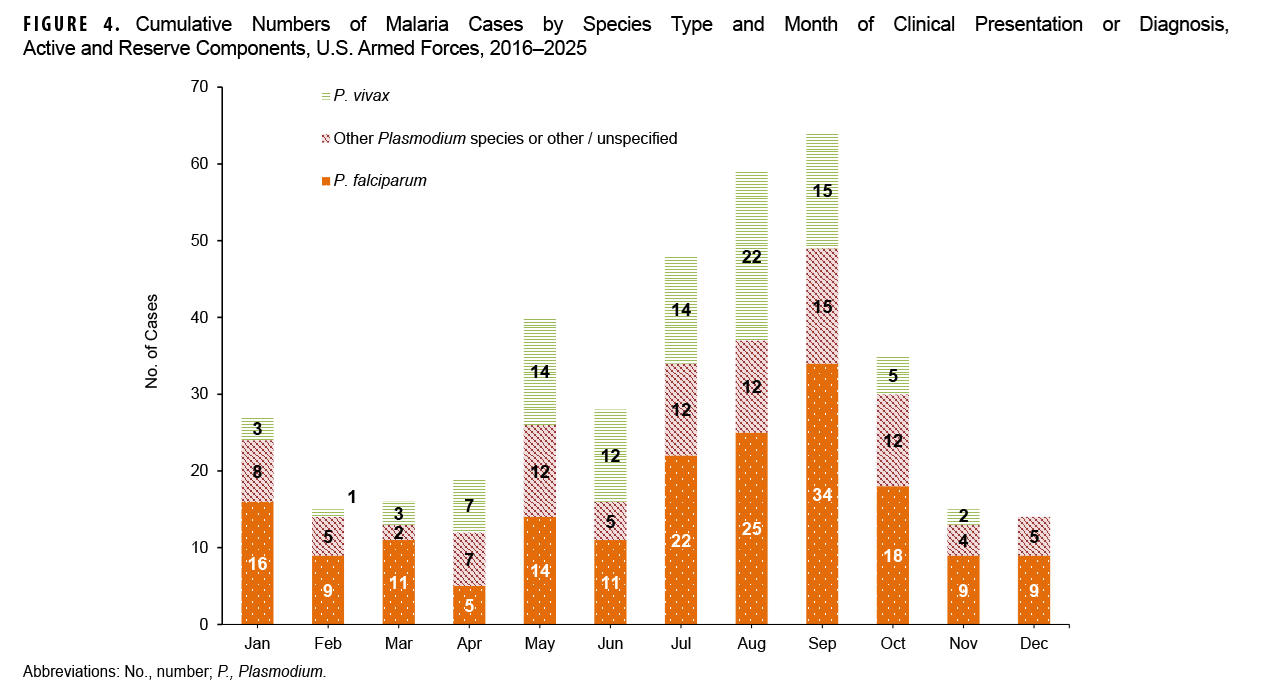
From 2016 to 2025, malaria caused by P. falciparum accounted for the greatest number of cases (183, 48.2%) followed by other or unspecified species (n=99, 26.1%), and P. vivax (n=98, 25.8%). Over the 10-year surveillance period, most malaria cases (n=274/380, 72.1%) were diagnosed or reported during the 6 months from the Northern Hemisphere middle of spring through the middle of autumn (i.e., May–October) (Figure 4). The proportions of malaria cases diagnosed or reported May–October varied by region of acquisition: Afghanistan (n=48/56, 85.7%,), Korea (n=58/65, 89.2%), Africa (n=117/169, 69.2%), and South and Central America (n=1/2, 50.0%) (data not shown).
Discussion
The number of malaria cases among U.S. service members saw a modest increase in 2025, rising by 12.5% from the previous year. While the total number of cases remains relatively low, these malaria data reveal several key trends and a notable shift in the dominant parasite species, underscoring the persistent threat of malaria to military personnel operating globally. Consistent with historical trends, the demographic profile of malaria cases in 2025 comprised predominantly young, male soldiers from the active component.3-5 The majority (77.8%) of cases were identified through routine RMEs, with the remainder captured through hospitalization and laboratory records, highlighting the importance of a multi-faceted surveillance strategy to ensure comprehensive case identification.
Geographically, Africa continues to be a primary region of acquisition for malaria infections, a consistent trend over the last decade.3 The majority of cases acquired in Africa were caused by P. falciparum, the most severe form of the parasite. Cases acquired in Africa were traced to at least 7 different countries, reflecting the widespread risk across the continent.
Perhaps the most significant finding from the 2025 surveillance data is the dramatic shift in the causative species. Nearly half of all cases were attributed to P. vivax, a stark contrast to 2024, when P. falciparum accounted for over half of cases—and P. vivax only 10%. This change is almost entirely driven by cases acquired in Korea, which accounted for 80% of P. vivax infections in 2025. This finding emphasizes the geographically distinct epidemiology of malaria and the specific risks associated with different operational theaters. This risk has long been documented since the Korean War, however, among U.S. and Korean Forces near the Demilitarized Zone.17
The seasonal pattern of malaria diagnoses remains consistent with previous findings, providing predictable opportunity for targeted force health protection measures. Over the 10-year surveillance period, a significant majority (72.1%) of cases were diagnosed May–October, coinciding with the warmer, wetter months that favor mosquito vector activity.18 This trend was particularly pronounced for cases acquired in Korea (89.2%), aligning with the established transmission season for P. vivax in temperate zones and reinforcing the need for heightened awareness and preventative measures during these months for personnel in those regions. Vector surveillance programs have shown a correlation between the number of Anopheles species positive for P. vivax sporozoites with the number of malaria cases and exposure of soldiers from the Republic of Korea soldiers from May through October.19 Even in Africa, where transmission can occur throughout the year,18,20 nearly 70% of cases were reported during this same period, underscoring its importance as a peak transmission season globally.
Limitations to this report should be considered when interpreting these findings. Malaria case reporting, especially for reserve components and non-deployment exposures, is likely incomplete, contributing to under-estimation of rates; some cases treated in deployed or non-U.S. military medical facilities may not have been reported or otherwise ascertained at the time of analysis. Malaria diagnoses documented only in outpatient settings without confirmatory testing and not reported as RMEs were not included in this report. Geographic location of malaria acquisition was estimated from reported information, with some cases reporting exposures in multiple malaria-endemic areas and others with no relevant exposure information. Personal travel or deployment to malaria-endemic countries was not documented unless specified in RMEs. Limited information on species types in RME records emphasizes the need for more complete attention to documentation of reportable conditions.
These findings emphasize the need for continuous surveillance, regionally specific prevention strategies, and robust diagnostic capabilities to protect U.S. service members from this persistent infectious disease. While the overall burden of malaria within the U.S. military is not significant, 2025 data illustrate a dynamic and evolving threat, with the continued prevalence of P. falciparum in Africa posing a significant risk for severe disease and the sharp increase in P. vivax from Korea demonstrating a different, but equally important, regional challenge.
References
- Shanks GD. Post-infection symptoms in U.S. soldiers with malaria during the Second World War: major limitation to return to duty. MSMR. 2026;33(2):8-10. Accessed Apr. 28, 2026. https://www.health.mil/news/articles/2026/02/01/msmr-malaria-post-infection-world-war-ii
- U.S. Centers for Disease Control and Prevention. Elimination of Malaria in the United States (1947–1951). U.S. Dept. of Health and Human Services. Jul. 23, 2018. Accessed Sep. 5, 2025. https://stacks.cdc.gov/view/cdc/100616
- Armed Forces Health Surveillance Division. Malaria among members of the U.S. Armed Forces, 2024. MSMR. 2025;32(4):22-28. Accessed Apr. 28, 2026. https://www.health.mil/news/articles/2025/04/01/msmr-malaria-2024-update
- Armed Forces Health Surveillance Division. Malaria among members of the U.S. Armed Forces, 2023. MSMR. 2024;31(5):31-36. Accessed Apr. 28, 2026. https://www.health.mil/news/articles/2024/05/01/msmr-malaria-update
- Armed Forces Health Surveillance Division. Malaria in service members and beneficiaries, U.S. Armed Forces, 2018–2022. MSMR. 2023;30(3):2-9. Accessed Apr. 28, 2026. https://www.health.mil/reference-center/reports/2023/03/01/msmr-volume-30-issue-3-march-2023
- Saunders DL, Garges E, Manning JE, et al. Safety, tolerability and compliance with long-term antimalarial chemoprophylaxis in American soldiers in Afghanistan. Am J Trop Med Hyg. 2015;93(3):584-590. doi:10.4269/ajtmh.15-0245
- Wallace MR, Sharp TW, Smoak B, et al. Malaria among United States troops in Somalia. Am J Med. 1996;(1):49-55. doi:10.1016/s0002-9343(96)90011-x
- National Academies of Sciences, Engineering, and Medicine, Savitz DA, Styka AN, eds. Assessment of Long-Term Health Effects of Antimalarial Drugs When Used for Prophylaxis. The National Academies Press;2020. Accessed Mar. 31, 2026. doi:10.17226/25688
- Miles D. Deployed servicemembers step up anti-malarial protections. American Forces Press Service. Apr. 9, 2004. Accessed Mar. 31, 2026. https://www.af.mil/news/article-display/article/137192/deployed-servicemembers-step-up-anti-malarial-protections
- Rudiger CL, Nowak G. Malaria trends in the Navy and Marine Corps, 2005–2013. Mil Med. 2016;181(5):488-493. doi:10.7205/milmedd-15-00174
- Helfrich AM, Lu D, Grance M, Chu X, Hickey PW. Malaria incidence in US military families is related to service member’s birthplace. Open Forum Infect Dis. 2025;12(8). doi:10.1093/ofid/ofaf479
- U.S. Centers for Disease Control and Prevention. Malaria. DPDx-Laboratory Identification of Parasites of Public Health Concern. U.S. Dept. of Health and Human Services. Updated Dec. 13, 2024. Accessed Mar. 31, 2026. https://www.cdc.gov/dpdx/malaria/index.html
- World Health Organization. World Malaria Report 2024: Addressing Inequity in the Global Malaria Response. World Health Organization;2024. Accessed Mar. 31, 2026. https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2024
- Howes RE, Battle KE, Mendis KN, et al. Global epidemiology of Plasmodium vivax. Am J Trop Med Hyg. 2016;95(suppl 6):15-34. doi:10.4269/ajtmh.16-0141
- Gething PW, Elyazar IR, Moyes, et al. A long neglected world malaria map: Plasmodium vivax endemicity in 2010. PLoS Negl Trop Dis. 2012;6(9):e1814. doi:10.1371/journal.pntd.0001814
- Armed Forces Health Surveillance Division. Malaria Surveillance Case Definition. Updated Feb. 2019. Accessed Mar. 31, 2026. Defense Health Agency, U.S. Dept. of War. https://health.mil/reference-center/publications/2014/12/01/malaria
- Feighner BH, Park S, Novakoski WL, Kelsey LL, Strickman D. Re-emergence of Plasmodium vivax malaria in the Republic of Korea. Emerg Infect Dis. 1998;4(2):295-297. doi:10.3201/eid0402.980219
- U.S. Centers for Disease Control and Prevention. Where Malaria Occurs. U.S. Dept. of Health and Human Services. Mar. 18, 2024. Accessed Apr. 8, 2026. https://www.cdc.gov/malaria/data-research/index.html
- Chang KS, Yoo DH, Ju YR, et al. Distribution of malaria vectors and incidence of vivax malaria at Korean army installations near the demilitarized zone, Republic of Korea. Malaria J. 2016;15:259. doi:10.1186/s12936-016-1301-y
- Yamba EI, Fink AH, Kingsley B, et al. Climate drivers of malaria transmission seasonality and their relative importance in Sub-Saharan Africa. GeoHealth. 2023;7(2). doi:10.1029/2022gh000698
Acknowledgments
The editors thank the Navy and Marine Corps Public Health Center–Portsmouth, for providing laboratory data for this analysis. The editors thank Gi-Taik Oh for analysis of the data presented in this report.
Disclaimers
The views expressed in this report reflect the results of research conducted by the authors and do not necessarily reflect official policy nor position of the Defense Health Agency, Department of War, or the U.S. Government.
The editors disclose use of an artificial intelligence (AI) language model in the preparation of this report. Assistance was provided by Gemini Enterprise, a large language model from Google, specifically optimized for Department of War mission support within an Impact Level 5 (IL5) environment. This AI application was used to assist with initial drafts of the discussion, to refine prose for clarity. MSMR editors directed all AI review and analysis, with subsequent editorial staff review and final edits. The editors assert full responsibility for the accuracy and integrity of the final content.