By Holly N. O'Reilly, Ph.D.
Feb. 25, 2022
 SAPRO graphic
SAPRO graphic
Some behavioral health providers may have questions about which treatments for sexual assault victims are the most strongly recommended by the VA/DOD Clinical Practice Guidelines, whereas others may want to know about the availability of treatment resources. The resources below are focused on the treatment of PTSD, but some survivors also report psychological symptoms of depression, anxiety or substance use. For more clinical resources visit the PHCoE Clinician Resources website.
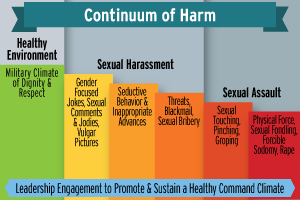
The Sexual Assault Continuum of Harm
The continuum of harm refers to a range of "inappropriate actions, such as sexist jokes, hazing, and cyber bullying that are used before or after the assault and or supports an environment which tolerates these actions."1 The most subtle forms of inappropriate behavior on the continuum include innuendo and jokes based on gender or sexuality. To paraphrase the Department of Defense Instruction 1020.03 Harassment Prevention and Response in the Armed Forces, sexual harassment may include unwelcome sexual advances, repeated comments of a sexual nature and/or requests for sexual favors which make an individual uncomfortable and imply that rejection of this behavior will lead to negative work conditions or career impact. For example, one of my former patients reported that his immediate supervisor made numerous sexual comments toward him, and when he stated that he was not interested, he was assigned undesirable duty hours and unpleasant work tasks. The most extreme behaviors on the continuum of harm include use of physical force and other types of sexual assault.
You may learn more from this sexual harassment blog.
There are also two important resources you may want to bookmark:
Trauma-informed care should be incorporated in all evidence-based treatment for the psychological consequences of sexual assault. Trauma-informed care is focused on principals rather than techniques to support the trauma survivor and their coping skills. The principles include: safety, collaboration, empowerment, recognition of family, peer support, trustworthiness and transparency and awareness of cultural, historical and gender issues. VA/DOD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder is a resource for trauma-informed care.
Providing Evidence-Based Treatment
The Department of Defense is committed to providing the best care for service members across mental health conditions. Jointly, the Department of Defense and Department of Veterans Affairs provide a series of clinical practice guidelines which are considered to be exemplary. The VA/DOD CPG for the Management of Posttraumatic Stress Disorder and Acute Stress Reactions is a guideline to support providers in their treatment planning. The CPG was developed by a team of subject matter experts and clearly describes the available evidence in support of treatments and the strength of their recommendation. The CPG provides strong recommendations for several of the treatments below, but encourages providers to use their clinical judgement and consider the patient's values and preferences when determining the treatment plan.
I would like to underscore that the CPG recommends clinical providers treat symptoms of PTSD with evidence-based treatments, even when the patient has co-occurring disorders such as depressive symptoms or substance use disorder. The CPG also recommends the use of cognitive-behavioral therapy for insomnia in patients who meet diagnostic criteria for PTSD.
Prolonged Exposure Therapy (PE)
PE is one of the first treatments effective in decreasing symptoms of PTSD. Treatment usually lasts for three or four months if sessions are conducted weekly, but there is emerging evidence of success conducting PE sessions more than once a week. PE teaches the patient to gradually approach trauma-related memories and other feelings or situations that have been avoided post-trauma. PE uses a cognitive-behavioral approach, has been extensively studied, and is used by many DOD mental health clinicians who have been trained in this method.2 For additional resources, see:
Cognitive Processing Therapy (CPT)
CPT is another of the earliest therapies effective for treatment of PTSD. It was originally developed to treat individuals with a history of sexual trauma, but has been shown to be effective across a range of trauma types. CPT is a cognitive-behavioral therapy which allows the patient to change the trauma-related thoughts they experience, which leads to changes in emotions. Like PE, the use of CPT has been extensively studied, many DOD mental health clinicians have been trained to deliver CPT, and it can be conducted individually or in a group format. Treatment usually is completed within three to four months. 2 For more information, see:
Eye Movement Desensitization and Reprocessing (EMDR)
EMDR is another treatment shown to decrease the symptoms of PTSD. EMDR was originally designed to reduce the emotional distress caused by traumatic memories. Theorists explain that EMDR allows the patient to access traumatic memories, process the emotional material, and reach an adaptive resolution. Like PE and CPT, this treatment has been used in numerous clinical trials with a variety of patients experiencing different severities of posttraumatic symptoms. Treatment is usually completed within twelve sessions, although some patients report relief much more quickly.2 More background can be found here:
Narrative Therapies
Several narrative therapies have been added to the list of manualized trauma-focused psychotherapies which are strongly recommended to reduce the symptoms of PTSD. These effective treatments include Brief Eclectic Psychotherapy (BEP), Present-Centered Therapy (PCT) and Interpersonal Psychotherapy (IPT). Unlike some treatments which teach the patients skills to tolerate the distress associated with PTSD, these treatments are designed to reduce the symptoms of PTSD. These short-term treatments are highly effective and can be used for patients disclosing multiple traumatic events.2 Additional details can be found here:
References
- Defense Research, Surveys, and Statistics Center. (2017). 2016 Workplace and Gender Relations Survey of Active Duty Members Overview Report (OPA Report No. 2016-050). Department of Defense. https://www.sapr.mil/public/docs/reports/FY17_Annual/FY16_Annual_Report_on_Sexual_Assault_in_the_Military_Full_Report_Part2_4.pdf
- The Management of Posttraumatic Stress Disorder Work Group. (2017). VA/DOD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder. https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal012418.pdf
Dr. Holly O'Reilly is a clinical psychologist and serves as the Program Manager for Sexual Assault Behavioral Health Clinical Intervention at the Defense Health Agency, Behavioral Health Clinical Management Team. She specializes in the psychological consequences of sexual assault and interpersonal violence.